
Understanding human behaviour in designing a future of health
In the future of health—where data and technology continue to advance exponentially—will human behaviour still prevent us from becoming a healthier society? How can we conquer the age-old problem of behaviour change both with and in spite of, technology?

Introduction
ALL around us, technology is making exponential advances in science and medicine. But despite these breakthroughs—in pharmaceuticals, diagnostics, precision medicine and health care delivery—seven out of 10 Americans are still expected to die from chronic disease.1
Though research suggests that many chronic diseases are preventable with better health behaviour, the structure, pace and inequities of society make health-damaging behaviour easy. We overeat and don’t get enough exercise. Our brains naturally favour foods with high levels of salt, fat and sugar. We know we shouldn’t have that extra glass of wine or binge-watch our favourite show and we don’t get enough sleep. We spend more time on social media than with friends and family.2
It is clear we need to change our behaviour. But behaviour change is hard, very hard and the cycle continues (figure 1).3

We engage in behaviours that are detrimental to our current and future well-being because we are human and irrational—but predictably irrational.4 Therefore, life sciences and health care organisations could benefit from a better psychosocial understanding of patients/consumers and the environmental and social barriers that keep people from being healthy. Many technology companies are already mastering consumer behaviour and are moving into health care.5
Health care and life sciences organisations should deliver a health care experience that is not only more precise—through the use of data and technology—but also more personalised. By making that experience more human, tailored to an individual’s specific needs and having an empathetic understanding of the challenges they face, we can begin to move society towards a culture of wellness and prevention.6
The imperative for health care stakeholders lies in helping consumers to:
- See the big picture and gain a holistic view of their health. A holistic view identifies the impact that daily choices have on well-being and can help foster better decisions—such as choosing to go to bed, instead of staying up for one more episode of a TV show.
- Make the big picture small and build self-efficacy. Even when motivated, changing something like diet or physical activity can seem overwhelming. Helping people determine where to start can be the difference between action and inaction. Setting smaller goals that are attainable can be easy wins that increase self-confidence and fuel greater and lasting change.
- Own their behaviour and make change sustainable. We tend towards optimism and overconfidence. Helping people be more realistic about their behaviour and abilities sets them up for more sustainable actions.
COVID-19, a catalyst for change, including behaviour change
The COVID-19 global health crisis is accelerating dramatic change.7 In addition to the devastating toll of the disease, the pandemic is changing the way we work and live. The event has been a catalyst for a future of health that otherwise might have taken years to attain,8 while at the same time, it is highlighting weaknesses in the system and diminishing consumer trust.9
Telemedicine is experiencing a record rate of adoption,10 and consumers are actively controlling their care through apps and websites.11 Recent Deloitte research shows consumers are taking charge more than ever before,12 and almost all clinical leaders (98%), have implemented or plan to implement virtual health practices for some or all nonprocedural visits.13 Some clinicians are specifically asking for training on how to conduct virtual visits and interact with patients.14
The pandemic is also uncovering serious deficiencies in our existing systems,15 and consumer attitudes and behaviours have been the focus of contentious debate.16 Without a vaccine or cure, the best defence is calling for worldwide behaviour change,17 including sheltering in place, frequent hand-washing, social distancing and wearing masks.18
Life has become a series of risk calculations.19 Those with comorbidities have a higher risk of becoming severe and fatal cases of COVID-19. Studies show hypertension to be more prevalent in those with severe cases and diabetes more prevalent among fatal cases.20 In addition to older adults and minorities, Hispanic, non-Hispanic Black and non-Hispanic American Indian/Alaskan Native children under 21 have been disproportionately affected by COVID-19, representing 78% of fatalities, according to the Centres for Disease Control and Prevention (CDC).21
In addition, governments anticipate a wave of mental and behavioural health issues could be on the horizon, including depression, substance abuse, post-traumatic stress disorder and suicide.22
Chronic disease and health care costs are rising
Most health care professionals are aware of the daunting statistics. Four out of 10 US adults have two or more chronic health conditions, and chronic disease for some racial and ethnic minority groups can be more common or severe (figure 2).23 As the population ages, the number of elderly with comorbidities is growing quickly24 as is the number of young people diagnosed with diabetes25 and heart disease.26

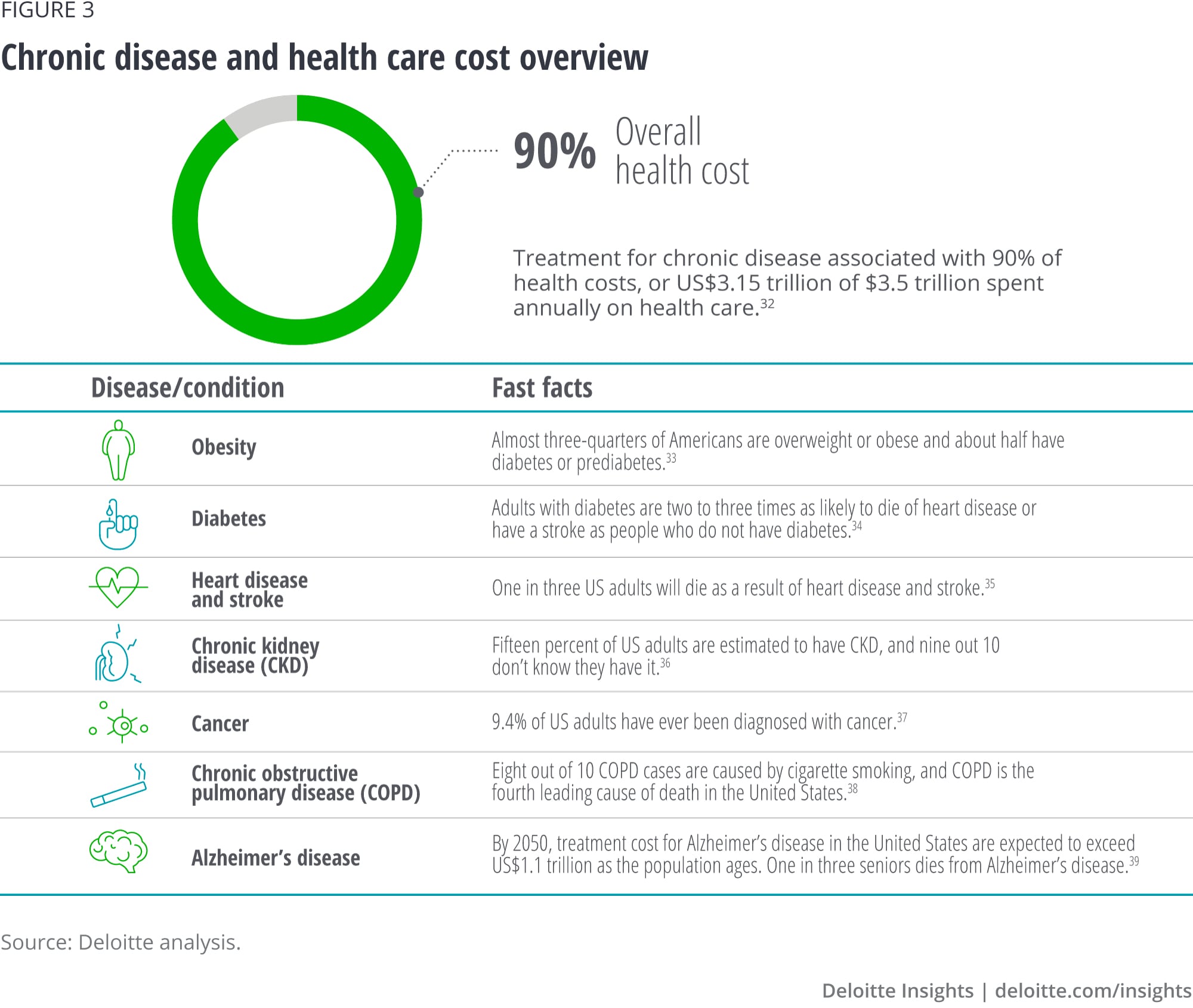
Health care costs are also rising and employers are shifting more health care expenses to employees, often through high-deductible plans (figure 3).28 By 2026, the cost of individual health care is expected to top US$16,000 per year. This individual total represents the amount everyone would pay into the health care system, including patients, the government and private health insurance.29
Because these high health care costs aren’t sustainable and aren’t always associated with better outcomes, we are seeing a shift towards value-based care. Instead of fee-for-service payment models that tend to incentivise fragmented, procedural care, value-based care places more emphasis on improving outcomes, expanding access to care, optimising costs and improving efficiencies.30
Driving real health outcomes requires an understanding of a patient’s health holistically, including the factors that shape their behaviour. Insurers and government are working on incentives for improving chronic disease management for beneficiaries and some clinicians find that they can help coordinate chronic disease management more effectively with the involvement of a social worker, behavioural therapist, or a nutritionist.31
There is much work to be done, but more engaged consumers and interoperable data may provide the impetus for health care stakeholders to take a closer look at behaviour change models and coordinated care. Companies innovative enough to test novel approaches to behaviour change can provide an evidence base that paves the way to a supportive health care system.

Behaviour is the foundation of health
Despite an increase in per capita health care spending,40 chronic disease continues to be the result of poor health behaviours. Research suggests that if behaviour-related risk factors were eliminated, at least 80% of all heart disease, diabetes and stroke could be prevented as could more than 40% of US cancer cases and deaths.41 Controlling these five health-related behaviours is key:
- No smoking
- Regular physical activity
- Limited alcohol consumption
- Body weight
- Sufficient sleep42
“Human behaviour is the final common pathway for the application of nearly every advance in medicine.”
—Mitesh Patel, M.D., director, Penn Medicine Nudge Unit43
Adopting a new approach, nuanced and adaptable behaviour change
Though health behaviour change is nearly guaranteed to improve health, knowing so doesn’t necessarily make it easy to change and sustain. That’s where the work of behavioural scientists can help. Behavioural science combines insights from psychology, anthropology, economics and neuroscience to explain how people choose to act under certain circumstances.44
While more than 300 behavioural teams have emerged over the last 10 years to provide insights for governments, businesses and other organisations,45 health care is just starting to catch on to the world of behavioural science.46 New nontraditional care providers, like Walmart and Amazon, have entered health care and have a wealth of consumer behaviour knowledge.
Challenges and barriers to behaviour change
Behaviour and lifestyle choices are heavily influenced by individual, environmental/structural and social/cultural factors.47 Once we identify these challenges and understand how they can influence behaviour, tools can be designed to work with, rather than against, human nature for healthy behaviour change.48
Individual factors
In today’s world, people have more information than they can process and when making decisions, many choose the quickest and easiest solution. Study after study demonstrates people opt for immediate gains over future rewards.49 This tendency, known as temporal discounting, may be offset by designing solutions that offer smaller rewards in the near term, rather than promising a larger reward in the distant future.50
Environmental and structural factors
The structure of our environment shapes our behaviour and our health. It’s difficult to expect people who live in food deserts and don’t have access to nutritious food to eat more fresh fruit and vegetables or to ask people to engage in telehealth without internet access or tools. The US Department of Agriculture (USDA) designates food deserts as low-income neighbourhoods that lack supermarkets and grocery stores.51
Even when following the same prescribed diet, health outcomes may be worse for people of lower socioeconomic status. In a recent study of the Mediterranean diet in Italy, researchers observed no benefits in a less educated, lower-income group, while cardiovascular risk factors were lowered in the more educated, higher-income group. This group had access to better quality and variety of fruits and vegetables and were more knowledgeable about and employed healthier cooking methods.52
Food is science and nutrition is not universal knowledge
Many may not know that cooking can either increase or decrease the bioavailability of some nutrients or that meal composition matters. Certain foods with fat-soluble vitamins are more easily absorbed if eaten with fats. Legumes, which are rich in protein and fibre, contain lectins that can impair the absorption of iron, zinc and calcium in other foods if eaten during the same meal.53 Choosing canned fruits and vegetables over fresh produce can add salt, sugar and additives that carry health risks of their own.54
Even physicians admit their training in nutrition is limited. The American College of Preventative Medicine believes that greater success in preventing chronic disease will happen when lifestyle medicine (LM) education starts in medical school.55 There is an urgent need to create and implement comprehensive LM education for health professionals, at all levels of training.56
Cultural and social factors
In the United States, our modern culture defaults to unhealthy behaviours. We are conditioned to seek instant gratification that is fuelled by technology.57 Our work culture is always “on” and connected. Research shows that almost two-thirds of US employees engage in unhealthy behaviours as a result of work stress.58 This has been exacerbated during the pandemic as many more people are working from home and struggle to balance work with disruptions to our way of life.59
Behavioralist Dan Ariely says that our work culture needs to change to value meaning and a long-term form of happiness.60 Lack of meaning is a psychosocial determinant of chronic disease.61 We can create more meaning when we treat people as useful and contributing. Too often, employees are asked to do tasks that are futile.62 We produce much more value when we can decide how best to accomplish our work63 and have a shared sense of purpose.64
“Understanding and cultivating our sense of purpose helps us find a deeper, more meaningful connection to the work that we do and how that work impacts the organisation, its people and our greater society.”
—Jen Fisher, director, Deloitte’s chief well-being officer
Cultural influences in a pandemic
Culture may affect why one patient seeks treatment or complies with medical approaches and another may not.65 Cultural norms may also play an important role in the way a country approaches a public health crisis like the coronavirus. Resistance to mask-wearing in the United States contrasts with behaviour in South Korea, where masks are an accepted protocol for dealing with a cold or flu and are becoming a fashion statement. When COVID-19 hit, mask adoption by South Koreans was widespread even before masks were required.66
Supportive technology for healthy behaviour
According to Deloitte's 2020 US Health Care Consumer Survey, 42% of US consumers said they use tools to measure fitness and track health-improvement goals. 67 Gen Z and millennials are more likely to believe trackers can change their behaviour, 68 and nearly two-thirds of those aged 14 to 22 report using health-related apps. 69 In 2020, the top apps by income include those for calorie counting, meditation and tracking exercise. 70
But technology alone does not work. For technology to be an effective part of behaviour change, it should include provider and social support or incentives.
Provider-supported technology, prescribing health and fitness apps
Increased access to telehealth and remote monitoring as a result of the pandemic is proving valuable to consumers. 71 These technologies have the ability to alter patient behaviour, so that patients can set healthy habits that stick. 72
Fitness and mHealth apps prescribed by a provider are also more effective. They were found to have 30-day retention rates 30% and 10% above average, respectively. 73 Without provider or social support, many health and fitness apps are quickly abandoned. In 2018, almost 85% of mHealth apps had less than 10,000 active users; only the top 7% reported more than 50,000 users. 74
Social incentives boost activity levels for wearable technology
Deloitte and the Perelman School of Medicine recently conducted a study on 602 overweight and obese employees utilising wearable fitness trackers. The trial, Social Incentives to Encourage Physical Activity and Understand Predictors (STEP UP), measured the effects of three different types of social incentives as well as gamification on increasing physical activity. 75
- The supportive arm asked participants to identify a friend or family member who was encouraged to support the participant in their progress during the study. They received weekly reports on the participant's performance, including the number of points earned and level achieved.
- The collaborative arm placed participants into teams of three and randomly selected a member each day to represent the team through their step activity. If this individual met the goal, the whole team was awarded points. The team lost points if the team member failed to meet the activity goal.
- The competitive arm had the highest engagement and most sustained improvement. It placed participants into groups of three and used a weekly leaderboard email to rank participants and foster competition in the group. 76
The STEP UP study found that all three groups with social incentives achieved more physical activity than the control group. This research illustrates how using data (progress tracking) and behavioural science (social incentives) together can impact change. These strategies may be employed to encourage other desired behaviours, such as healthy eating or improved medication adherence. 77
Moving to the future of health for behaviour
A shift is occurring gradually, but it can have a tremendous impact on traditional health care players. In the future of health, patients will likely own their data, more easily share it with third parties, 78 and use it to play a central role in health care decision-making. Start-ups are already making it possible for individuals to sell their health data for clinical research. 79
With shared information and a more holistic picture of a person’s health, technology is identifying health risks early and helping move the focus to well-being and prevention, rather than treatment. Technology can also enable more precision engagement and personalised health experiences as a result of accessible data and AI.
But more data and technology in the hands of nonclinical decision-makers could lead to bad decisions. Consumers will likely need more support to interpret health data and guide their decision-making as well as help to develop systems and skills that can change their unhealthy behaviours.
Addressing decision-making failures
Solving the reality-intention gap in decision-making
How do people make decisions? Nobel laureate and behavioural economist Daniel Kahneman in his popular book, Thinking, Fast and Slow, says people think and make decisions based on two systems:
- "System 1,"which is fast, instinctive and emotional
- “System 2,"which is slow, more deliberate and rational 80
Kahneman says that a whopping 98% of our thinking is System 1 thinking. 81 Thinking (mostly) fast leads to “reality-intention gaps,” according to Jason Riis, chief behavioural scientist of Behavioralize, who studied under Kahneman. Reality-intention gaps are misperceptions of the world that create inconsistencies between reality and our intentions to thrive.
Riis says that bridging these gaps is not easy, but progress is possible. Usually, it requires more than giving people “better information,” and instead, internalising some new concepts that change the way we make inferences and judgements. Developing a “growth mindset” is an example of such a change.
Individuals should understand both why a change needs to be made and how to make that change. 82 With a growth mindset, individuals also believe that the potential for change is possible and they work harder to change unhealthy behaviours. 83 By keeping track of small wins, these individuals may gain a healthy sense of pride for their accomplishments and motivation for the long term. 84
Deloitte recently conducted a Critical Thinking and Future of Health Survey that found that health consumers are overconfident and underestimate how often they make critical-thinking errors (figure 4). Only 43% of young consumers reported making critical-thinking errors daily or weekly. This seems unlikely considering the frequency of risky behaviours (e.g., not wearing masks during the pandemic, dangerous driving, eating poorly, etc.).
Given the number of choices people face, it is hard to imagine anyone could go a day without making a critical-thinking error. Yet few consumers see it this way. People think others are more prone to error than they are (with 53% suggesting others make errors daily or weekly), another form of overconfidence. Interestingly, overconfidence was even higher for older participants, with only 20% estimating they often make critical-thinking errors.
Health systems should understand consumer decision-making beliefs and processes. To prevent critical-thinking failures, providers should find ways to support better reasoning and self-reflexion—providing “better information” will not likely be enough.

When asked about worries related to future health problems, survey participants were more frequently concerned about outcomes of disease—such as health expenses and lifestyle limitations—rather than the future risk of having the disease itself. This finding offers a practical suggestion for patient materials that aim to associate present health behaviours with future health risks. Such materials may have a greater impact if future risks are described in outcomes that people can more easily imagine and relate to, such as not being able to work or enjoy their typical activities.
In helping people with decision-making and self-reflexion, Riis suggests asking more insightful questions and emphasising health outcomes versus future disease risk. This shift can better inform health and wellness interventions. It may also help consumers make better inferences and self-reflect on their beliefs and behaviours.

In addition, providers should consider asking questions about patients’ perceptions of health and their future self. While the vast majority of patients have been asked if they smoke, drink and are physically active, very few report being asked about their future health or related worries (Figure 5). Indeed, more people have been asked (by a provider) about their favourite TV show or film (22%) than about how healthy they think they will be at age 50 (15%).
Understanding bias
In addition to critical-thinking errors, health consumers tend to approach decision-making through cognitive biases that are typically unconscious and automatic. For example, we may think we understand something when all we have is general familiarity. We experience a knowledge illusion, says Riis. We may think we know what’s risky and what isn’t and we may be wrong.
Many people are also in denial.85 They don’t see themselves as a number in the daunting statistics for chronic disease.86 “Not me,” they believe. This optimism bias keeps individuals from taking preventative measures for their health.87 Even when faced with a diagnosis, many patients think they are healthier than they really are.88
Decisions may also be faulty because they are based on preexisting beliefs. With confirmation bias, people only look for information that confirms what they already know.89 More than 100 different types of cognitive bias can prevent us from making good decisions.90
Health consumers will likely need help addressing their individual biases and decision-making failures. Having their data is not enough. They should work with providers who can lend their expertise and support in making sense of that data and their behaviours.
Designing a health care experience for human behaviour change
Developing an empathetic health care experience
Humans thrive on empathy,91 and empathy is becoming central to chronic disease management and health care delivery.92 Clinical empathy is an intellectual understanding of the emotions of others and part of patient-centred communication93 to understand individual, cultural, environmental and social factors, such as social determinants of health (SDOH).
Empathising with patients94 and genuinely caring for their experience and well-being builds trust.95 According to Deloitte’s 2020 Survey of US Health Care consumers, a trusted clinician relationship remains paramount.96 Patients who trust their clinicians are more likely to be honest, less defensive and follow treatment plans for lifestyle changes.97
“Empathy and compassion have been shown to change physiology, reduce pain and mortality, increase adherence and reduce health care costs. Empathy is the cornerstone of creating ‘therapeutic alliances’ between the health care team and patients.”
—Summer Knight MD, MBA, managing director, Deloitte
If we want to build a more human health care experience, health care professionals will need training to become more empathetic clinicians. Interestingly, Deloitte research found that US physicians want this type of training.98 Empathy is also becoming part of medical school training and continuing education99 and may even become a factor in medical school admissions.100
Reimagining primary care
Experts believe primary care should be redesigned to give equal attention to physical and behavioural health. To focus efforts on health promotion and disease prevention, they also suggest moving wellness into the primary care setting.101
However, a lack of confidence in their ability to offer lifestyle counselling hinders some clinicians and many feel they are stretched too thin. Primary care physicians (PCPs) may be better served by a health care delivery model that is team-centric and includes:
- Physicians trained in lifestyle medicine
- Health care coaches
- Psychologists102
Some experts suggest behavioural professionals should co-lead the primary care team and their self-care expertise can be a bedrock for expanding primary care services.103 Others suggest placing the community health worker—not the PCP—at the centre of the care team to address social determinants that drive health outcomes.104
Using adaptable technology to enable health behaviour change
In the next decade of consumer-driven health care, life science and health care organisations will likely need a nuanced and adaptable approach to behaviour change that can address consumers’ needs in a personalised way.105 Making technology adaptable means creating microinterventions tailored to individuals, employing behavioural archetypes and leveraging accessible data and AI to personalise engagement. Designing technology that can meet the customer wherever they are–and in a way that they prefer–can be a key to behaviour change.
Creating microinterventions tailored to individuals
One key to successful behaviour change is developing habits that make change easier. Productive habits have specific goals and are measurable.106 Because habit change is a process, succeeding with smaller goals along the way aids consistency. Health care stakeholders can help guide patients through the process by finding the right microintervention for each patient.107
In Tiny Habits: The Small Changes that Change Everything, Stanford behavioralist B. J. Fogg says that small changes can lead to bigger change. By making behaviour changes really small, they become easier to do and are automatic.108
Fogg suggests tying a new behaviour to an existing one. You may decide to floss just one tooth right after washing your face in the morning. Fogg finds that people may start with one tooth, but quickly start flossing more.109 Another example is turning off your phone right after you open the door to your home after work. By making this action automatic, it becomes easier to take a break from technology and focus on more meaningful things, like family or exercise.110
Small changes are easy to instigate with an alert and are ripe for technology-based interventions that are similar to consumer-based personalised marketing systems. Making healthy choices easy is the foundation to an effective nudging system.
Nudging through environmental changes is another type of microintervention. Healthy choices can be presented in a way that makes them easy and automatic (if not the default), reducing consumer effort when adopting healthier behaviours. Research shows that making a relatively subtle change to the food environment (i.e., presenting the salad separately from unhealthier foods) has a positive impact on food choice.111
Sensing technology that meets consumers wherever they are
Chronic disease management is becoming more connected via sensors, telehealth and remote patient monitoring.112 In the future of health, more consumers will likely use smart personal and medical devices and seamless, invisible platforms to help manage their health and wellness, wherever they may be.113
Passive data analysis on these sensors, including on mobile health technologies, can yield insights into consumer patterns that affect health. It may also be the easiest way to insert a nudge (e.g., channel, timing and message).
Cityblock brings adaptable technology and Neighbourhood Hubs to underserved communities
Cityblock delivers primary care, behavioural health, chronic disease management and other health services under one umbrella to patients in underserved neighbourhoods. The startup addresses social determinants of health, such as transportation, housing and access to healthy food.114
Cityblock’s technology platform, Commons, allows for all members of a patient’s care team to be aware of an individual’s health status and events. Technology is also used to empower people to have a role in their own care.115 Care teams are available 24/7, wherever it is convenient for the patient—at home, in the community, at their neighbourhood hub, or virtually. Hubs are built to meet local community needs and provide a space for members and care teams to meet.116
Employing behavioural archetypes
Organisations can increase the effectiveness of behaviour change initiatives by designing applications and offering incentives that are tailored to consumer types. This could involve gaining a better understanding of the characteristics of people who share similar behaviours and the barriers that may keep them from healthy behaviour. Then, strategies or nudges can be developed to address those groups.
Archetype analysis can also use behavioural patterns over time to identify groups of patients who behave similarly in the course of their care journey. Using this type of analysis on data from Clinicas del Azucar (CdA), the largest private network of diabetes and hypertension clinics in Mexico, Deloitte showed that the care provided in these “one-stop shops” for diabetes care resulted in lower HbA1c levels, but it requires patient engagement.
By reviewing patient health care data over time, Deloitte and CdA identified three main groups based on engagement patterns. Working with both CdA staff and patients, Deloitte also identified specific barriers to continued engagement for patients in these groups—cost, attitudes, or self-confidence. Tailored strategies could be developed to help keep them engaged in care.
Deloitte’s STEP UP data is being analysed to identify classes of patients who are most likely to respond to incentives as well as the behavioural archetypes that can help in the development and matching of incentives. The results will be published in the near future.
Leveraging accessible data and AI to personalise engagement
Clever technologies can make health care more mobile, portable and affordable and enable the delivery of the right solution at the right time, personalised for an individual health consumer.117 Interoperable data provides better access to patient information and health care is starting to use artificial intelligence (AI) for precision engagement, tailoring nudges to an individual’s personality, motivations and challenges.118
Tailored nudges (choices and interventions) are possible in real time (when it matters most) using adaptive reinforcement learning methods. Traditional analytics and data science methods work at the population level, comparing people with similar demographic profiles to suggest what might work. It’s not the same as building a personalised model that is based on an individual’s previous behaviour; it identifies factors most likely to influence that decision and is responsive to actions taken (choices made).
Personalised testing can also be combined with reinforcement methods to shape approaches and interventions that may work best for an individual. When we observe how someone handles a particular decision, we gain a powerful data point and can test different derivatives to inform our understanding of that individual. This creates a virtuous, personalised cycle.
Investing in health behaviour
“Because of COVID-19, every business leader is thinking about health and knows it is a core part of business continuity. The life sciences and health care industry must respond to the crisis today, while also helping us thrive after COVID-19 with improved health behaviour, mental health/resilience and employee wellness.”
—Asif Dhar, US National Life Sciences & Health Care Industry leader, Deloitte
Change is a process and every company should assess its ability to meet challenges and determine the building blocks necessary for supporting healthy behaviour. While an organisation’s business model and populations of interest will likely guide decisions, areas to consider should include investments in talent, infrastructure and data security, and partnerships.
Making the right investments in talent
Designing with people in mind requires talent and expertise in behavioural science. With their extensive knowledge, behavioural scientists can help close the gap between scientific and business communities and bring psychological principles to business and marketing strategies. New C-suite roles are emerging.119
- The chief behavioural officer (CBO) is a leader skilled in applying behavioural science and has an in-depth understanding of business and customer challenges. CBOs are advocates for keeping people at the centre of policies and programmes and are responsible for journey-mapping the consumer experience to behaviour and motivations. Bloomberg predicts that the top jobs for the next decade will be behavioural scientists and data analysts.120 In addition to being a curious problem-solver, the CBO ideally possesses a talent stack that includes:
- Experimental design
- Psychology knowledge
- Data analysis
- Digital experimentation
- Product management121
- The chief experience officer (CXO) is a leader who oversees both customer experience (CX) and employee experience (EX) holistically. Great employee experience is often the foundation for great customer experience.122 Deloitte’s CXO, Amelia Dunlop, leads a team of problem-solvers who use human-centred design and customer insights strategy to help businesses shift their focus from customer experience to human experience.123
“We believe that people want to be treated like humans and less as a part of a homogenous customer experience. Designing for a human experience is a bigger opportunity.”
—Amelia Dunlop, chief experience officer, Deloitte Digital124
Making the right investments in infrastructure and data security
Infrastructure investments should focus on flexible, adaptable technology and using data insights to create AI-powered personalised interventions. This usually requires access to workflow for training models directly on human responses and proposed interventions. Most analytical infrastructure exists outside of health care workflow and partnerships are often required.
AI-powered insights at an individual level require individualised interventions and tests—exponentially straining legal and regulatory review processes not designed for rapid and personalised, multivariate testing. AI methods also often struggle to support documentation and validation processes designed for population-level intervention programmes. Investments in AI and data technology should be coupled with innovations in legal and regulatory review processes (often improved through a different application of AI).
Health care stakeholders should also couple data and analytics infrastructure investments with a modern data governance model. A modern model allows for role-based (and, specifically, data scientist) access to de-identified datasets for testing in sandbox environments. Governance should cover data, insights and algorithms.
Finally, data security is a dominant concern for health consumers and it should remain front and centre for health care and life science organisations. With so many new and evolving sources of data, we need methods and technologies that protect that data and predict and prevent attacks. While minimising risk, organisations also need to be sensitive to the ethical use of health data.
Making the right investments in partnerships
Partnerships are a pillar in transforming 21st century health care. They call for a joint approach to solving problems while empowering the consumer at the centre of the health care ecosystem. They should also involve the communities where patients live, work and play.125
Consumers
Organisations should consider how to earn the trust and partnership of consumers, especially considering the amount of sensitive health data being generated around patients and the bioethics of health data.
Communities/community organisations
Community organisations and patient advocates can help address social determinants of health and structural issues. They are a trusted voice that brings unique insights about the populations they serve and can drive human-centred solutions to health challenges.
Strategic business partnerships
Strategic business partners elevate the whole to a sum greater than its parts. For example, when CVS acquired Aetna, the retailer combined its knowledge of consumer behaviour with the insurer’s data warehouse containing rich information on health care costs, quality and utilisation patterns. The result was both optimisation of care delivery and consumer engagement.126 Also, consider the brand permission that strategic partners bring to the relationship—specifically, do they have the trust of consumers and the public?
Technology ecosystems
Technology ecosystems help drive decision-making, but players come and go. When designing and building solutions over the long term, health care and life science organisations should be able to adapt to unanticipated changes. New sources of data and platforms should be plug-and-play and foster interoperability.
Academia
Researchers can help identify promising technologies and develop new methods for applying research findings to health problems. Their breadth and depth of research may help determine the likely success of approaches. Researchers are also training the next generation of talent and can be a great resource for acquiring new talent.
Government and policymakers
Government services and policymakers are sources of vast amounts of public health data and knowledge. They can help identify new and overarching problems. Partnerships in these areas can forge a joint interest in shaping policies that can impact health behaviour (e.g., land use, food taxes, screening requirements).
Conclusion
Health behaviour has been a persistent problem and not one that is going to be solved in the short term. But behaviour is the foundation of health and should be addressed. We cannot look to technology and technology disruptors alone to fix the health behaviour problem. Instead, we need to acknowledge and address the infrastructure and drivers of poor health behaviour at every level, from the individual to societal level.
These changes cannot be made overnight and will likely require investments and partnerships that will build value over the long term. Behavioural science and a human approach should be built into nearly every aspect of health care delivery and drive the design of health technology, not vice versa. Paired together, there can be tremendous gains to be made.
We can build a better future of health if we keep individuals and the human experience at the centre of initiatives. An empathetic health care system that realises people are wired to make unhealthy decisions can gain the knowledge it needs to drive better health outcomes and a healthier society.
Strategy checklist: Adopting a behavioural science approach
To enable consumer-driven health care based on behavioural science, we should assess our current approach and resources and set the direction for the next decade. How will you reorient your approach for the future of health? Are you asking the right questions?
- Helping consumers make good decisions
- How can data be presented for better decision-making? Are we addressing well-understood and identifiable decision-making failure modes (e.g., overconfidence, affective heuristic, etc.)?
- Do we understand the cognitive load and health literacy requirements implicit in our communications? Is there a formal (and quantitative) approach to evaluation of messages and offers as related to cognitive load?
- Is there a two-way exchange of information between us and consumers? Can the consumer provide feedback and correct our data? Can we adapt messages, interventions and/or incentives to consumer feedback?
- Designing engagement and experience for humans
- How can we create a more empathetic health care experience? Are our investments in technology making the experience more human, more personal? And does the experience adapt and improve over time for consumers?
- How can we make behaviour change more intentional? Are we helping people break down large long-term goals into smaller, nudgable steps that build self-efficacy and can be the start of a habit-formation model?
- Are we really working towards a 360-degree view of consumers, or do we just use the term to feel better about integrating our customer interaction data? Specifically, how much investment (if any) have we made in understanding the consumer as they and their relationships, understand themselves?
- Can we tie our investments in engagement to quantifiable improvements in satisfaction and experience? Can we report: “We’ve seen a 20% improvement in experience associated with the ‘$’ spent on ‘x’ last year?”
- Effectively applying adaptable technology that enables personalisation
- Are we using AI as a better analytical mousetrap (e.g., shifting from logistic regression to ElasticNet) or are we thinking about AI in consumer and business workflow? Where is the “artificial” in your AI investments—where are we mimicking the human process and influencing decisions and outcomes?
- Do we have a clear vision of a personalised experience? What is the role of data and technology in that vision?
- Investing in talent and partnerships
- Who is focussing on building and maintaining an empathetic human experience?
- What companies have brand permission with consumers for us to take the relationship with consumers to the next level?
- What partnerships can we put in place to accelerate development (and fail fast)? Who is more agile than we are and how can we partner with them for speed?
The future of health
The health industry is on the cusp of a major transformation that will affect all stakeholders. Incumbent players can either lead this transformation as innovative and well-connected market leaders or they can try to resist this inevitable change. A wide range of companies—from inside and outside of the health care sector—are already making strategic investments that could form the foundation for a future of health that is defined by radically interoperable data, open and secure platforms, and consumer-driven care.


{kind=link}