
Amplifying Black voices
What health care organizations can do to advance diversity, equity, and inclusion in the workforce
Improving DE&I among the health care workforce is an important component of ensuring health equity. Research by Deloitte and NAHSE aims to ascertain where the industry is in terms of DE&I in the workforce and what it can do to improve performance.
Executive summary
Health equity is a top concern among health care executives,1 and many recognize that their organizations must close gaps in health disparities by focusing in part on diversity, equity, and inclusion (DE&I) in their own workforce. Deloitte’s recent research on health care executives’ perspectives on health equity showed that many executives see the strong connection between diversity and inclusion within their workforce and improved health equity outcomes among patients. A diverse and inclusive health care workforce—both in clinical and nonclinical/corporate settings—can help improve trust and empathy and strengthen the connection with patients and communities.
Joint research by the Deloitte Center for Health Solutions and the National Association for Health Services Executives (NAHSE) on the current state of DE&I initiatives in the health care workforce showed that health care leaders recognize that improving DE&I in the workforce can support quality of care and financial performance goals. Addressing racism and other biases can give organizations a competitive advantage, helping them attract the best talent and elevate their brand and reputation.2
We sought to put forth evidence-based considerations for health care organizations seeking to address DE&I within their workforce and the communities they serve. What must organizations do to recruit and retain diverse talent, build a diverse workforce, and confront systemic racism to help improve health equity in their patient and member populations and communities?
Deloitte and NAHSE surveyed 105 NAHSE members and interviewed 10 executives at health care organizations who are leading DE&I initiatives in their workforces (see appendix for more information on the methodology). Topics covered included personal experience working in health care, organizational priorities and strategies around DE&I, and opportunities in career advancement. We found that in many areas of DE&I, health care organizations are moving in the right direction and have achieved much. However, they risk having many different initiatives and activities without making sustainable, meaningful impact. The survey data and findings from our interviews showed that while organizations are prioritizing DE&I initiatives in the workforce, more work needs to be done to engrain it in the culture and build on the current momentum:
What is working
•Most NAHSE professionals reported that their organization’s leadership respects individual differences, encourages collaboration, and recognizes the importance of diverse perspectives.
• Two out of three respondents agreed that their management and leaders encourage them to continue with their professional growth and development.
• DE&I initiatives are widespread, funded, and connected to business priorities:
- Four in five respondents reported their organization had active DE&I committees or was launching initiatives.
- 61% of these organizations had funding directed toward these initiatives/committees; while three in four respondents said these initiatives were connected to the organization’s business priorities, indicators that these initiatives are not just ways of “checking the box” but are becoming engrained in organizations’ strategic direction.
What can be done better
• Two in three respondents felt that all employees have not been fairly treated regardless of differences in backgrounds or beliefs or were neutral on this question; more than one in three felt that the recognition of their impact is diminished as a result of differential treatment based on gender, race, and/or ethnicity.
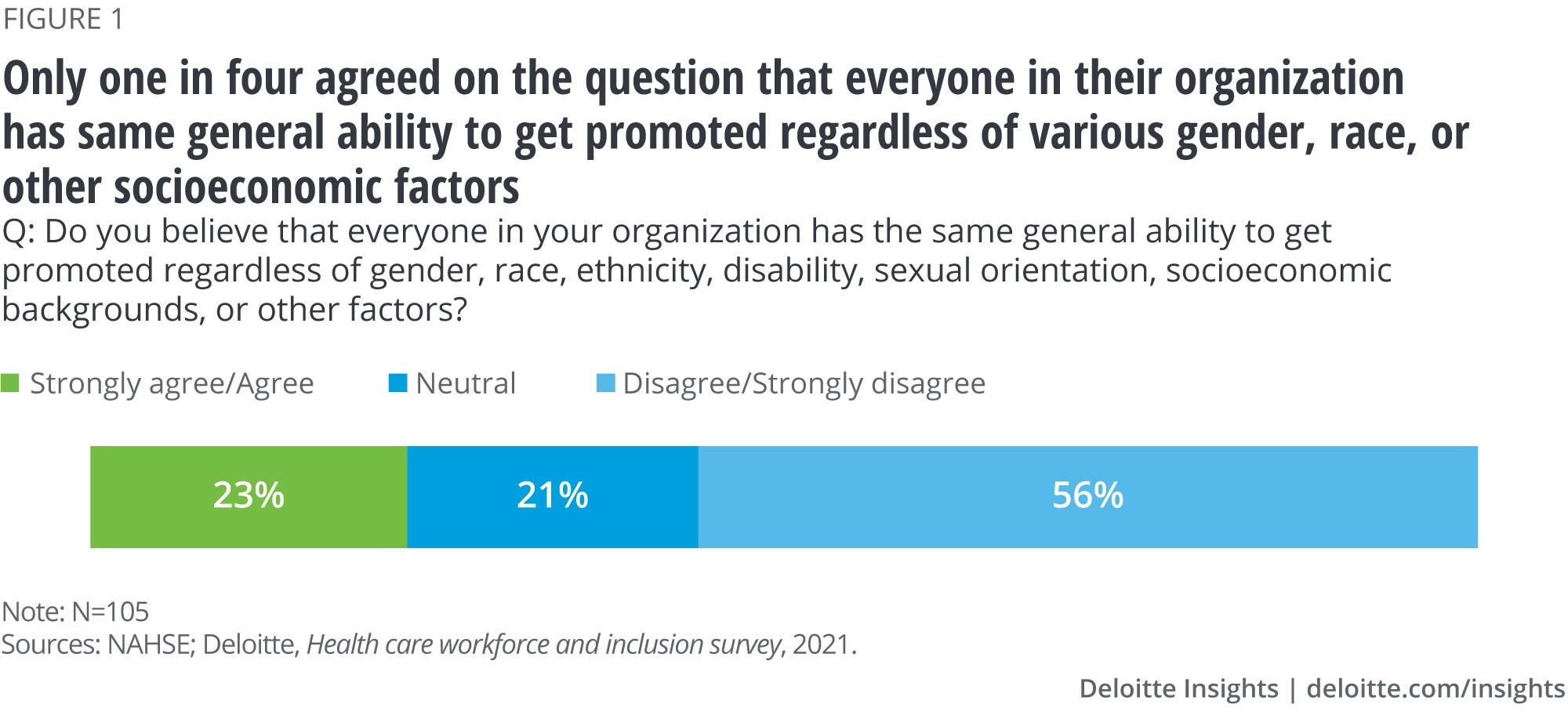
• Three in four respondents did not believe that everyone in their organization has the same general ability to get promoted regardless of gender, race, ethnicity, disability, sexual orientation, socioeconomic backgrounds, or other factors.
• Accountability and meaningful measurement around DE&I are lacking, as are initiatives around antiracism.
- Three out of four respondents did not believe that leadership is held accountable for meeting the objectives and goals of the DE&I committees.
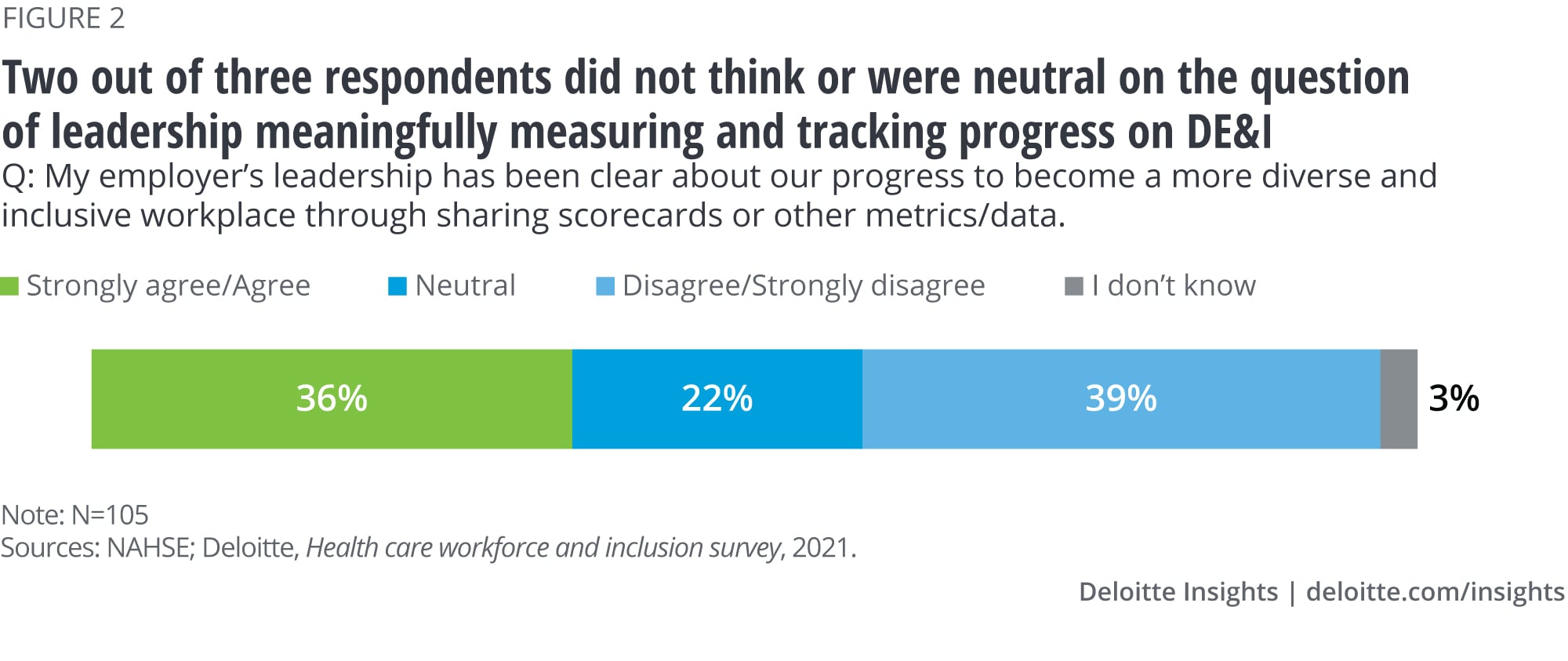
- Two out of four thought that leadership was not meaningfully measuring and tracking progress.
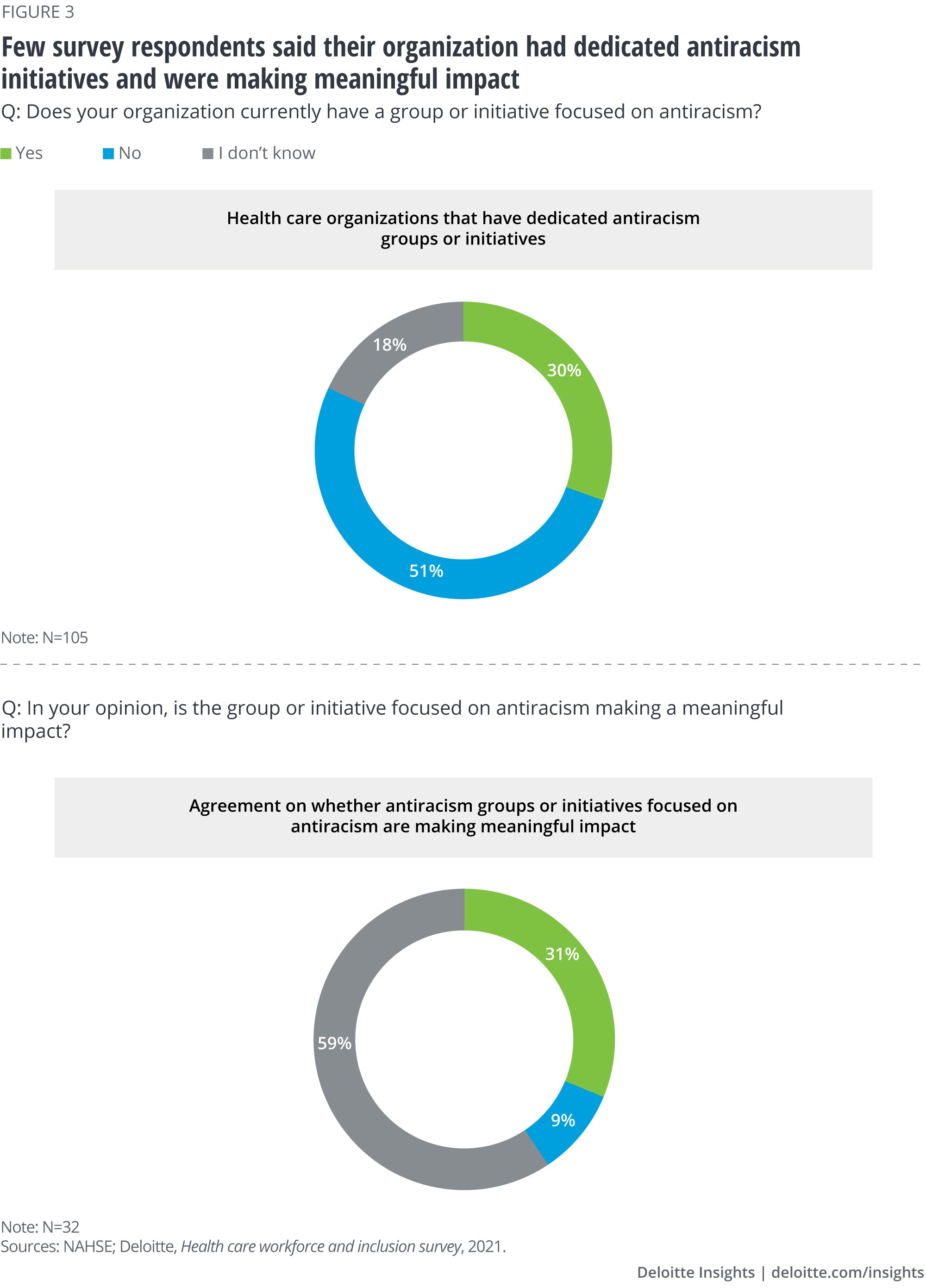
- Four out of five reported their organization did not have antiracism initiatives.
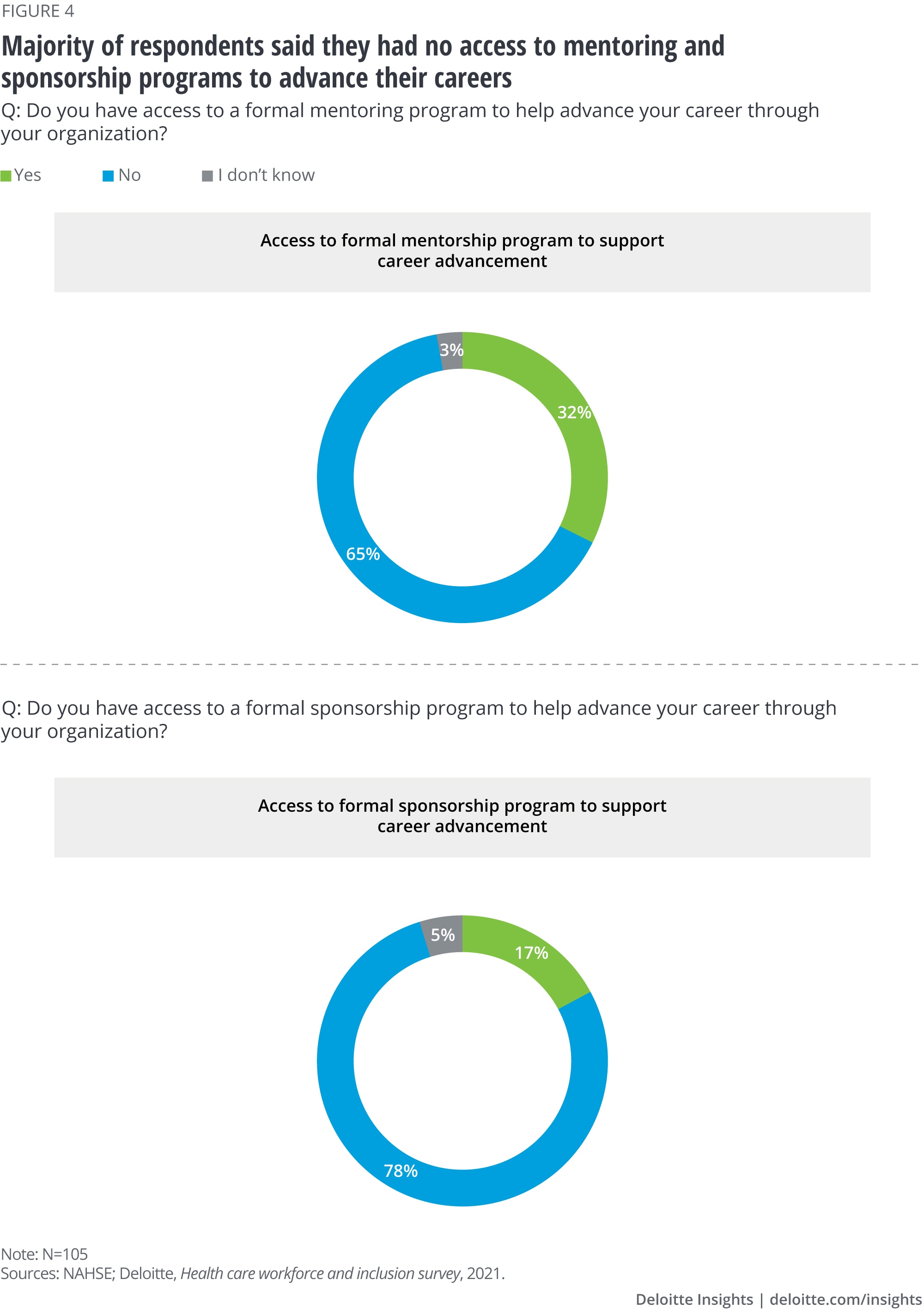
• Mentoring and sponsorship programs are deficient, withtwo in three respondents reporting not having access to mentoring programs while three in four said they did not have access to sponsorship programs.
Our findings show that DE&I initiatives in health care organizations are gaining traction and DE&I in the workforce is a top priority. But for these initiatives to make a sustainable and meaningful impact, health care leaders should consider the leading practices we identified around operationalizing DE&I, getting to meaningful measurement and benchmarking, and building effective mentoring programs that help retain and grow top talent and diverse perspectives.
Operationalizing DE&I in the workforce: How leading organizations are building impactful and sustainable initiatives
Defining diversity, equity, and inclusion
Diversity: The characteristics with which we are born and gain through experience, both seen and unseen, that make us different and similar.
Equity: The outcome of diversity, inclusion, and antioppression wherein all people have fair access, opportunity, resources, and power to thrive with consideration for and elimination of historical and systemic barriers and privileges that cause oppression.
Inclusion: The actions taken to understand, embrace, and leverage the unique strengths and facets of identity for all individuals so that all feel welcomed, valued, and supported.3
There is a strong body of evidence that DE&I is good for business. It fosters innovation, creativity, and empathy in ways that homogeneous environments rarely do,4 and these are important for organizations aiming to help patients and communities get and stay healthy. Hospital C-suites and boards remain largely white, even as Black, indigenous, and people of color (BIPOC) are an increasingly large part of the patient population. Just 14% of hospital board members and 9% of CEOs are minorities, according to the most recent study by the American Hospital Association’s Institute for Diversity and Health Equity—a number that has remained unchanged from 2013. At the same time, BIPOC constitute about a third of hospitals’ patients, and that figure is growing.5
In the fall of 2020, NAHSE and the Deloitte Center for Health Solutions researched the state of DE&I in the health care workforce. We sought to find out how health care organizations can engrain DE&I into the culture and fabric of the business. What are some leading practices for ensuring health care organizations preserve and build on their DE&I efforts, and ultimately, get to better health equity in their patient populations and communities? We put forth evidence-based recommendations on how health care organizations can move forward to build sustainable, meaningful initiatives that can change the trajectory of DE&I.
Lessons from our research
Four strategies to operationalize DE&I in the health care workforce
Our survey showed that while many health care employees feel respected and think that leadership is making DE&I in the workforce a business priority, leaders could be doing more to make them feel everyone has the same opportunities for advancement regardless of background, race and ethnicity, gender, and other factors (figure 1). Leaders can also be held to higher accountability standards and be more transparent around the metrics they are using to measure progress toward a more diverse, equitable, and inclusive workforce.
Interviewed chief diversity officers and other operations and strategy leaders stated that as health care organizations create and implement DE&I initiatives, they should also include cultural competency initiatives and training on unconscious bias. They should hardwire DE&I by making it part of the onboarding process; through continual training; and by tying it to employee reviews, performance measurement, and compensation. Leaders were also proud of their organization’s efforts toward DE&I, but many fear that DE&I efforts and progress could slip away with changes in leadership and shifting priorities. According to many of these leaders, the sustainability of these initiatives is at risk.
Leaders believe that at every turn, health care organizations should connect DE&I initiatives with business priorities. One leader gave us a specific example of how his organization added to its business case. The health system had market share in certain areas, but that was starting to erode as competitors moved in. He thought that the health system needed diverse perspectives to think through strategies for attracting and retaining patients in certain areas of the market. The old ways of thinking were not working anymore. To reach different markets, leadership knew they had to identify strategies to look at new ways of attracting and retaining diverse talent, and ensure that their workforce had a deeper understanding of the different markets they were trying to reach.
Four critical strategies to operationalize DE&I and ensure sustainability include:
• Make DE&I enterprisewide—involve the entire C-suite rather than house it solely in human resources (HR)
• Cultivate employee resource groups through executive sponsorship
• Get serious about DE&I when looking at talent and leadership pipeline
• Measure—and lead with data
Leaders were also proud of their organization’s efforts toward DE&I, but many fear that DE&I efforts and progress could slip away with changes in leadership and shifting priorities. According to many of these leaders, the sustainability of these initiatives is at risk.
Make DE&I enterprisewide
In our survey, 61% of respondents reported that their organizations were directing funding to DE&I initiatives. While there is clearly room for improvement, it shows that a fair number of organizations are dedicating resources to these initiatives and not just trying to check the box.
One chief diversity officer talked about the importance of dedicated DE&I resources versus shared resources. For example, the team had to wait for funding for certain initiatives it wanted to roll out. They were told that learning and development would get around to the new trainings the DE&I team wanted to roll out when funding was available, which was not empowering and threatened to slow down progress.
While many of the interviewed leaders at organizations where DE&I initiatives were based out of HR thought this could be limiting, some thought the initiatives could thrive here, especially if the C-suite itself was not diverse. Most leaders agreed that if DE&I is independent of HR, these initiatives can move beyond being exclusively about talent. All agreed that regardless of where the initiatives sit, organizations need to think through how they can broadly and deeply scale DE&I without marginalizing it to one part of the organization.
Cultivate employer resource groups through executive sponsorship
More than 80% of the surveyed employees reported that their organization had committee(s) or task force dedicated to DE&I priorities. Though we did not ask specifically about employer resource groups (ERGs), leaders talked about the importance of having leading practices for ERGs. These are voluntary groups led by employees, which aim to foster a diverse, inclusive workplace aligned with the organization. They comprise employees at all levels, including housekeeping and food service.
They said each group should have an executive sponsor,6 who may not be a member, but is responsible for helping remove barriers for members. If leadership is mostly white men, then white men should be part of these conversations for change to occur, since they are the current leadership. If organizations are assessing DE&I through surveys, one leader said that these groups should also collect more qualitative data through dialogue. Aggregated themes that arise from these dialogues should be shared with leadership.
Get serious about DE&I when looking at talent and leadership pipeline
Some leaders said they heard hiring managers complain about not being able to find a diverse workforce. But this complaint is often unfounded. In reality the organization is often not looking in the right places. One leader said minority women in health care might not be aware of opportunities in the business side of the industry: “Hospitals have traditionally been a bit of a boys’ club. There are a lot of white males in leadership. Black women might not gravitate toward the corporate side of health care.” She went on to say that her career accelerated when she was approached in nursing school to consider a leadership development program. Health care organizations should be proactive about educating underrepresented minorities and women about opportunities in health care beyond clinical roles, and then follow up with programs that can help them grow and develop leadership skills. Being proactive about developing and nurturing diverse talent within the organization shows that leaders are investing in their people. It may also help organizations retain roles such as chief diversity officers, which have notoriously high turnover, in part because of factors such as unrealistic expectations and lack of support from senior executives.7
Other leaders talked about the need for organizations to dig deep into their recruiting and hiring process to root out bias. Training in implicit bias for everyone, especially those who have hiring responsibilities, is critical. Having multiple people review all applications to ensure that strong applicants don’t fall through the cracks in residency programs and nonclinical/corporate roles at all levels is also important.8 One leader told us their organization blocks out applicants’ names for certain corporate-level positions to prevent bias when reviewing resumes.
Measure—and lead with data
Few respondents to our survey thought that their health care organization was measuring and tracking progress toward becoming a more diverse and inclusive workplace (figure 2). To manage something, one should define the objectives, measure and track progress, and communicate findings. If having a more diverse and inclusive workforce is the goal, then organizations should think about what those targets might be, and what the timeline is. Leaders we interviewed stressed that measurement and reporting9 were critical to the sustainability of DE&I initiatives.
Examples of metrics organizations should consider include:
• Recruitment (breakdown of who applied and was interviewed) and hiring
• Promotions
• Retention and turnover
• Employee engagement—through surveys, focus groups, and ERG discussions
• Compensation and bonus
• Supplier and vendor diversity
Return on investment (ROI) metrics might include market share and revenue, cost savings from retention, linking employee engagement scores to productivity.10 Leaders believe that once the organization has the metrics and data, it should be transparent. Many mentioned the importance of dashboards and reporting data both internally and externally.
Leaders also emphasized the importance of setting bold goals and using data to tell the story. One health system saw a 6-year difference in life expectancy between a low-income area and an affluent area just 6 miles away. This was a powerful data point that got people’s attention and helped guide the organization in setting goals around improving health outcomes: to reduce the gap by 50% in the next 10 years.
To track progress, organizations should understand the baseline. It’s ideal to have preintervention data, but if that’s not available, organizations could explore benchmark data from others in the industry. Another leading practice is to set clear goals and agree on them. One leader asked, “If only 20% of senior management candidates are diverse hires, is that okay? What is acceptable? Leadership has to agree and that drives your direction.”
Another leader discussed the challenges of measuring ROI for DE&I: “We get stuck in loops sometimes when it comes to demonstrating value. In business school, we learn you have to show ROI, show the value. It can be hard to do in this space. You might have powerful stories of patient impact, but it’s hard to measure what didn’t happen when it comes to prevention or getting ahead of something in terms of keeping patients out of the emergency room.” The leader said that having an independent entity such as one of the nonprofit think tanks or health care research organizations might help take on this challenge for health systems.
One health system saw a 6-year difference in life expectancy between a low-income area and an affluent area just 6 miles away. This was a powerful data point that got people’s attention and helped guide the organization in setting goals around improving health outcomes: to reduce the gap by 50% in the next 10 years.
Antiracism initiatives are still uncommon
Less than a third of survey respondents said their organization had specific antiracist initiatives among their DE&I initiatives. Of those, less than a third thought these initiatives were making a meaningful impact (figure 3).
It has been noted that prior to the pandemic and George Floyd’s murder, many companies were striving to be nonracist, but not necessarily antiracist.11 Being nonracist is not enough. Because this is new terrain for many organizations, it is not surprising that these initiatives are not yet making a meaningful impact. In time they might. But how does an organization become an antiracist institution?
Leaders said their organizations were focusing on specific trainings and informal conversations. They might start with explaining that antiracism is not about excluding anyone, but rather being unapologetic about including others. Training topics included unconscious bias and inclusive leadership. One organization was experimenting with modules where employees were presented with workplace incidents. They rated how comfortable they were in their responses. Then a heat map was created around the responses to show employees areas where they had assumed they had made an antiracist response when in fact they had not.
Some of the organizations hosted informal conversations where employees shared personal stories where they dealt with racism. One leader told us that her coworkers were shocked to learn that she makes a conscious effort to dress and present herself in a certain way when she goes out, to avoid being uncomfortable or in danger. They were shocked because she is a well-educated C-suite professional with a high income. “They assumed I was shielded,” she said. In these conversations, employees need to hear what it means for them to be silent versus what it means to be an ally.
Few professionals reported having access to formal mentoring and sponsorship programs in their workplace, though leaders we interviewed thought these were critical.
Surveyed professionals said there was a dearth of formal mentoring and sponsorship programs. Two out of three professionals had no access to mentoring programs, while three in four lacked access to sponsorship programs (figure 4). During 2020 and most of 2021, many nonclinical/corporate health care professionals worked remotely at least some of the time. Most of us have not been gathering in person. It might be more challenging to offer these programs in a virtual environment, but it’s just as important to continue them.
Every leader we interviewed talked about the critical role of mentors and allies in their own lives and careers (“You have to have people willing to kick down doors on your behalf”). They spoke about people they looked up to when they were young or starting their careers (“You can’t be what you don’t see”); about people who told them of opportunities they never would have otherwise heard of; about mentors who showed them the unwritten rules of conduct; and about those who helped them deal with unconscious bias (“You need someone to be your wing woman. To make sure you don’t trip”).
Deloitte’s research shows formal mentoring programs should use professional and personal aspirations as criteria to match employee with mentors.12 A mentor often acts as a confidant, shows the way to navigate workplace challenges, and has the “hard talks.” Mentoring should serve to help organizations identify high-potential employees and ensure they are provided with the resources they need to develop and feel supported. A sponsor should be an experienced senior-level person who advocates for the advancement of the individual by providing exposure and engagement with senior leaders. A sponsor should be willing to advocate for and “bang the table” for advancement and growth.
Mentoring across the organization—via peer networks—is another leading practice. People within ERGs can network and learn from each other. Sponsors of ERGs can help employees prepare to lead and boost confidence. The idea of reverse mentorships is that the benefits can go both ways, and more experienced leaders can get more exposure to employees of different generations, races, and genders, which can help eliminate unconscious bias.
As with every initiative related to DE&I, organizations should measure their mentoring and sponsorship initiatives by establishing key performance indicators and tracking them over time. Expectations, metrics, timelines, and outcomes should be clearly laid out, and accountability for meeting them established. Leaders should hold each other accountable through routine check-ins and reports that focus on continuously improving programs. Finally, organizations do not have to solely focus on internal mentoring programs. Many of our interviewees mentioned partnering with external organizations that can help their employees build and grow their careers.
Health care organizations can’t do it alone: Big changes are needed at federal and state policy level
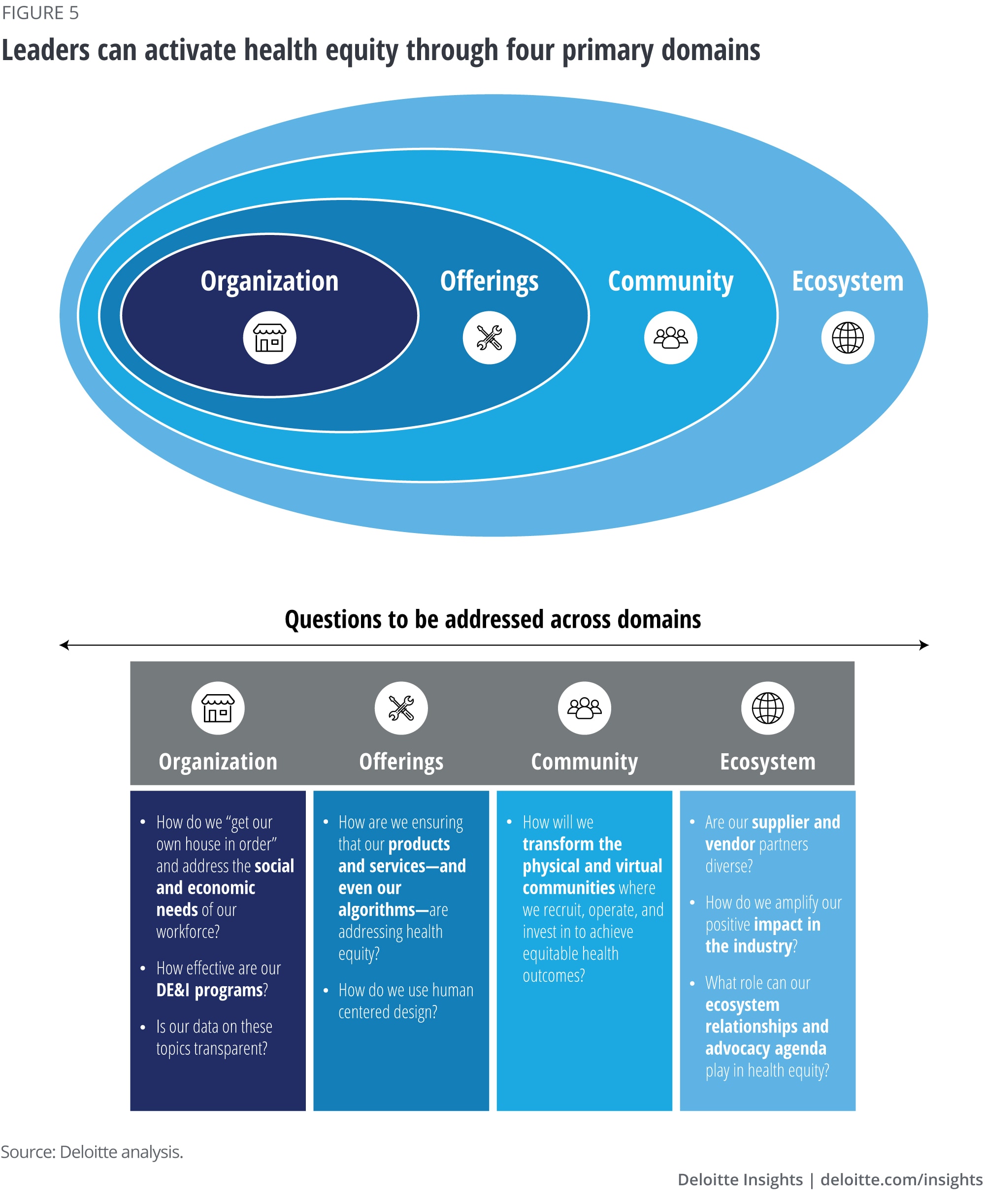
Health care organizations clearly have a major role in advancing DE&I in health care, and the goal of our research was to focus on domain one of the four domains of health equity that Deloitte has identified in our health equity framework (figure 5):13 the organization, whichrefers to how an employer addresses DE&I in the workplace.
Our interviewees discussed the importance of DE&I being a part of the culture of their organization to improve offerings to the patients and members they serve. One leader told us that every health care organization should pay a livable wage and ensure employees have access to high quality, affordable childcare. He mentioned that there is a continuing education infrastructure for physicians, but why shouldn’t cafeteria workers and other lower wage employees have access to educational opportunities? Many leaders also noted the importance of vendor review selection and of making certain criteria a contractual obligation.
Leaders also spoke about the importance of community initiatives, including how some large employers were making corporate pledges to increase diversity in employment and leadership by defined metrics and to hold each other accountable. Others talked about the increase in partnering with atypical partners. One health system is partnering with a bank on certain community initiatives because economic empowerment in the community is critical. Part of the initiative centered around increasing investment in diverse businesses and helping the community increase financial literacy.
Beyond the four walls of their organizations, leaders want to see more broad changes in their community, and the larger ecosystem. A major barrier to real, systemic change is that as a society, we tend to look for individual, singular solutions to address holistic and structural problems.14 To impact their communities and the larger ecosystem, the leaders spoke about the need for the United States to address economic disparities and the racial wealth gap, policing inequities, educational inequities, and environmental injustices that disproportionally affect BIPOC and racism in health care. These are not small issues that can be summed up neatly or quickly. But leaders believed that starting in their own workforce, with their own leadership and employees, is a critical step to branching out to address inequities and racism in their patient and member populations and in their communities.
Appendix
Methodology
NAHSE and Deloitte designed and fielded an online survey to more than 2,000 NAHSE members in March 2021. A total of 105 respondents completed the survey.
• Our respondents were mainly Black women (91% of the sample identified as Black, and 68% identified as women).
• Respondents ranged from C-level/executive management (22%), senior management (29%), mid-level management (30%), and entry-level/nonmanagement staff (8%). The remaining 12% were physicians, nursing leaders, or clinicians.
• Most respondents worked at hospitals or health systems (57%), with 10% coming from universities or academic institutions, and the remaining respondents working at health care associations, medical device and digital health companies, and health plans.
We also interviewed 10 executives who are leading DE&I initiatives at health systems and health plans working at NAHSE member companies. These leaders included chief diversity officers, chief operating and strategy officers, and human resources executives. Topics covered in both the survey and interviews included personal experience working in health care, organizational priorities and strategies around DE&I, and opportunities in career advancement.
Deloitte’s Services for the Health Care Industry
Amid uncertainty and change, health care stakeholders are looking for new ways to transform the journey of care. By focusing on the differentiated needs of plans and providers, our US Health Care practice helps clients transform uncertainty into possibility, and rapid change into lasting progress.
