Addressing health care’s talent emergency
Stabilizing the industry’s staffing shortage should start with redesigning the work model, investing in people, and rebuilding trust in leadership.
Executive summary
The US health care industry is facing an unprecedented staffing shortage, particularly among frontline clinicians. The workforce is increasingly burned out, overworked, and unsatisfied. They’re working extended hours and have limited coverage for time off—and they’re walking out in droves to explore new opportunities or exiting the workforce altogether. Although these issues aren’t new or unique to health care, the immense physical and emotional strain of the COVID-19 pandemic has brought them to the surface. And the result is a true talent emergency—one that requires urgent action from all health care leaders.
To understand what steps health systems should take to address the talent emergency, the Deloitte Center for Health Solutions conducted two streams of research to examine the problem from multiple perspectives and identify short- and long-term solutions. From April to June 2022, we interviewed 29 US industry experts, including health system executives responsible for clinician well-being, operations, human resources, and strategy, as well as nursing and medical administrators, scholars, and policy advisors. In August 2022, we surveyed 500 US frontline clinicians who currently or recently practiced in acute and ambulatory settings including, 250 nurses, 170 physicians, and 80 advanced practice providers.
The talent crisis has begun to attract more attention: The Office of the Surgeon General and a few industry groups have issued statements and made appeals to the industry to address burnout among health care workers.1 Developing long-term solutions requires a thorough understanding of the problem—and how it has evolved. Until recently, approaches to improve well-being targeted individual factors such as employee resiliency.2 There is now broad recognition that organizational and systemic factors—work design, culture, workforce supply, and policy—are major contributors to worker burnout, which, in turn, leads to worker shortages.3
To address the underlying drivers that have led to the talent emergency and achieve a long-lasting impact, our research shows that health systems should fundamentally transform the way they deliver care. It's time for the industry to acknowledge that old tools have outlived their usefulness and that we need innovative approaches to how clinicians work, who they work with, and where they work. While redesigning the work should be at the center, these transformation efforts are unlikely to succeed without making ongoing investments in people and rebuilding trust in leadership.
Reimagine care delivery and redesign the work
Chronic burnout is proof that clinicians’ jobs are unsustainable, and the industry cannot continue with the status quo. Yet, our survey data suggests that the status quo is the norm. Surveyed clinicians gave their organizations a grade of “C–” on their efforts to address burnout. The respondents identified many unnecessary and low-value tasks that take time away from patient care, such as those that satisfy administrative requirements (32%) and work that could be done by others or automated (20%), yet they have low expectations of their organizations to innovate.
Most of our interviewed experts, on the other hand, stressed that the path forward involves a complete care model transformation and job redesign. Specifically, they recommend:
- Investing in technology to give time back to workers. For instance, optimizing clinicians’ workflows by getting rid of low-value activities, such as reducing the number of electronic health record (EHR) clicks, can be a quick win. Leveraging automation to reduce time spent on nonclinical work probably takes longer to produce results, whereas new work modalities, such as virtual nursing, that take advantage of remote work possibilities and lessen demands on bedside nurses are longer-term investments.
- Fundamentally rethinking where care is delivered. As more care moves out of hospitals and into outpatient and other alternative sites of care, be smart about staff allocation and preparation and design staff development programs accordingly.
- Redesigning work teams. Implement comprehensive interdisciplinary care teams that take advantage of team members’ strengths, bring in more assistive clinical workers, and allow everybody to operate at the top of their license.
- Injecting flexibility into jobs. The solutions range from flexible schedules and job-sharing to work models that formalize opportunities to intermix bedside work with other types of work.
Invest in your people
Interviewed experts and surveyed clinicians reminded us that because care delivery is a fundamentally human experience, care transformation efforts require investing not only in technology and processes but also in people. Several experts even warned that “we can’t automate our way out of this crisis,” while calls for better staffing were a common refrain in the survey responses.
If satisfaction with compensation and benefits is an indicator of how workers feel about their employers’ investments in their people, our survey results point to a glass-half-full scenario: About half of frontline clinicians are satisfied with their compensation (44%) and benefits (51%). They also say internal career mobility is challenging: Forty-two percent of frontline clinicians find it difficult to change roles inside their organization, one-third (33%) say it isn’t possible, and only 25% say such opportunities are available.
From our interviews, we learned that to attract and retain workers, health care organizations should balance extrinsic and intrinsic rewards, and recognize and accommodate cultural, generational, gender, and life-stage differences. Several forward-thinking organizations spoke of efforts to design opportunities for career advancement and mobility that match employees’ current and future needs.
Interviewees also called for continued investments in workers’ well-being and resources to support self-care, whereas frontline clinicians asked for additional resources to back up those programs—for example, providing enough staff coverage to allow employees to use their paid time off and truly disconnect from work.
Restore trust in organizational leadership
For many organizations, the first step is convincing the leaders to conduct an introspective and honest assessment of their own actions. How well are you caring for your clinicians?
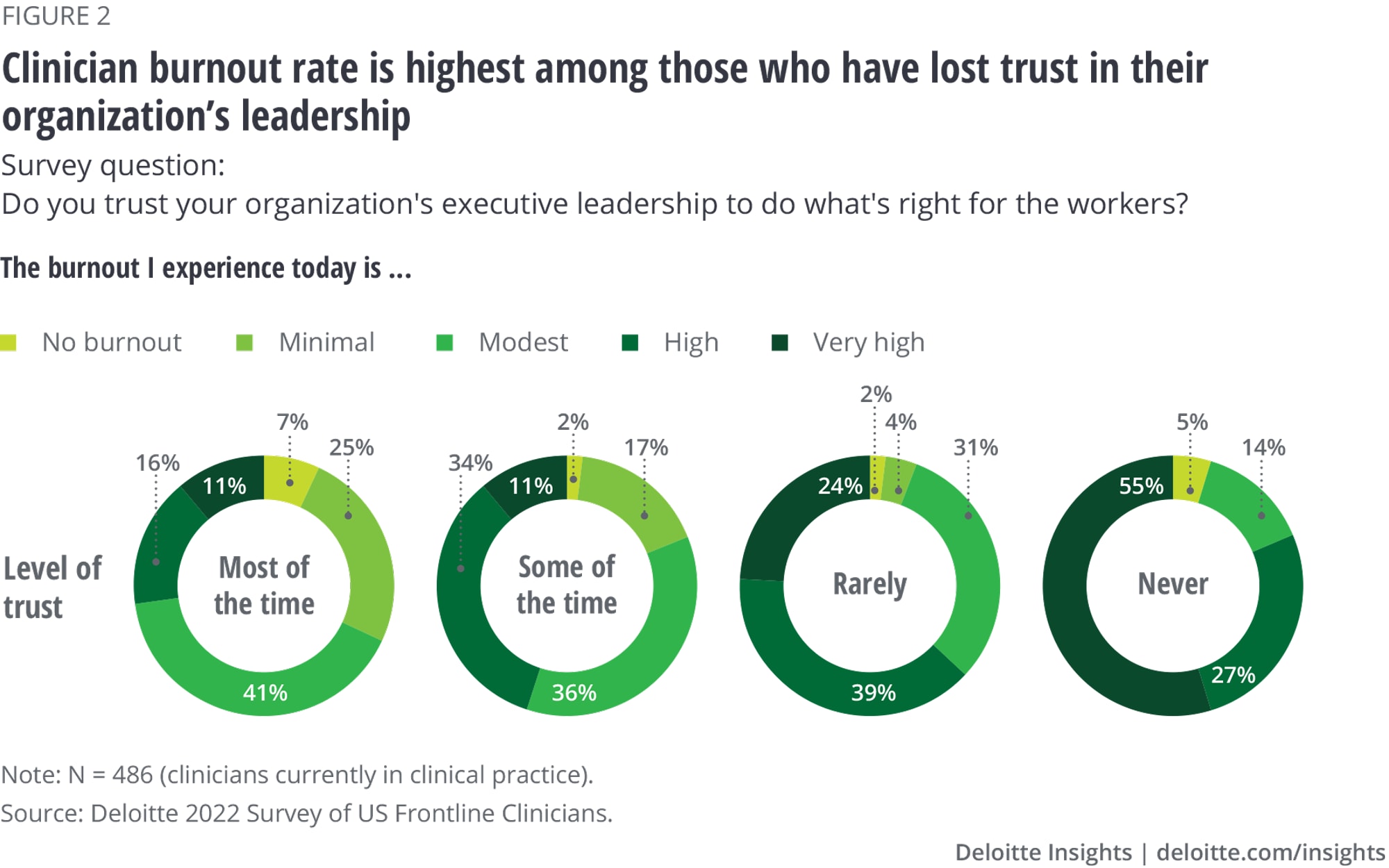
Our survey reveals that fewer than half (45%) of frontline clinicians trust their organization’s leadership to do what’s right for its patients. Even fewer, 23%, trust their leadership to do what’s right for workers. These two types of trust—to do right by patients and to do right by workers—are highly correlated and associated with significantly lower clinician burnout.
To retain and attract the clinical workforce, health care leaders have a responsibility to rebuild their trust and restore meaning, value, and purpose in their jobs. Listening to frontline workers, recognizing their clinical autonomy, elevating their voice to leadership, and building an inclusive culture are some ways organizations try to achieve this. Holding leaders accountable for worker well-being—by weaving well-being metrics into their compensation and creating leadership positions focused on well-being—can further solidify leadership’s commitment to their workers.
Establish a strong path forward
Frontline clinicians and industry experts are alarmed by the effects clinician shortages have on the quality of care and their ability to deliver on the mission. At the same time, they see this as an opportunity to innovate, learn from each other, and create workplaces and a system of care that can enable patients and clinicians to thrive in the Future of HealthTM.
This mandate to reinvent care delivery comes at a time when margin pressures make it incredibly hard to commit to long-term investments. While hard choices and tradeoffs will be required, perhaps margin improvement programs don’t have to be antithetical to clinician experience. It could be possible to design them in ways that don’t just optimize the costs but also improve population health and enhance the experience of receiving and providing care.
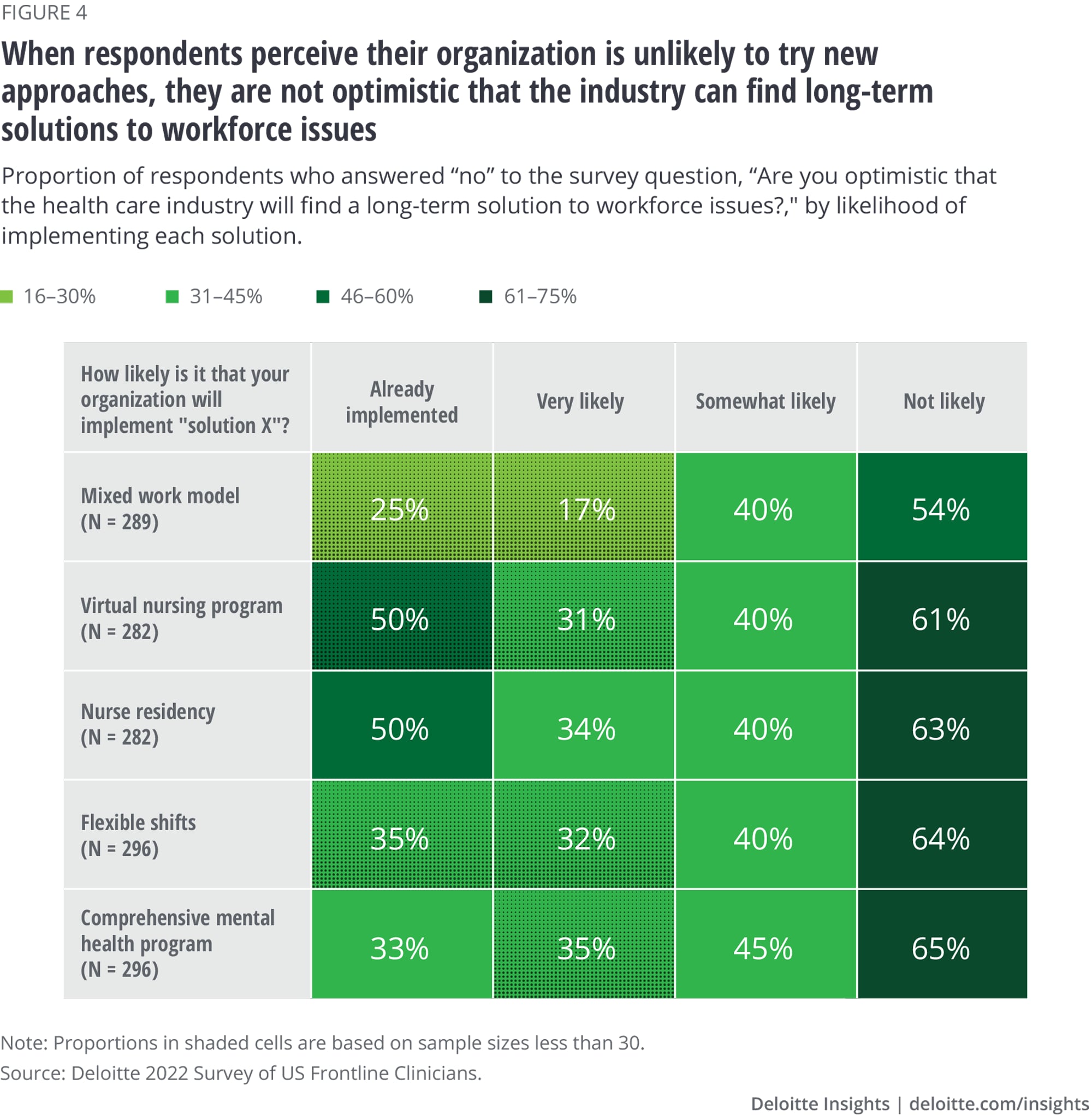
Our findings give us hope: Even though frontline clinicians are largely pessimistic that the industry can find a long-term solution, the outlook is significantly brighter in workplaces where respondents perceive the appetite to implement innovative solutions. We interpret this as a sign that the industry is capable of innovating and can garner the goodwill to commit to long-term strategies to solve the talent emergency and avert future crises.
Introduction: The clinician shortage is industrywide
Today, health care organizations are facing an industrywide talent emergency due to unprecedented levels of burnout and attrition that led to shortages of frontline clinicians (and health workers more generally).4 Our survey results paint a dire picture: About half (46%) of the clinicians reported high levels of burnout, 35% said their burnout is modest, and only 19% reported no or minimal burnout.
For health care organizations, the shortage of health workers is a complex problem, with several underlying causes. Research shows that numerous organizational and systemic factors—such as work design, culture, workforce supply, and policy—are responsible for frustration, dissatisfaction, and burnout.5
Clinician shortages are a strain against organizations’ missions to serve patients and the community. After years of steady decline, the incidence of health care–associated infections significantly increased in 2020, according to CDC analysis. Researchers cite staffing shortages and high caseloads as some of the reasons for this increase.6 Several other recent studies point to a link between workforce shortfalls and increases in patient safety events.7 Researchers have long warned of burnout and staffing shortages as threats to high quality and safe care.8 In our survey, almost all clinicians are concerned that health care worker burnout (98%) and shortages (99%) can result in decreased quality of care in their communities.
The public is also increasingly aware of the problem and concerned about how it could impact their health. The Deloitte 2022 Survey of US Health Care Consumers found that four in five (82%) consumers are aware of the health care worker shortage. And about seven in 10 are concerned that the worker shortage may affect their own health, and that of their families (67%) and communities (69%).
As more burned-out clinicians leave their organizations or health care altogether, the industry has responded with tried-and-true tactics like leveraging existing workers to work overtime and using staffing agencies to fill in gaps. However, we’re beginning to see the limitations of this old playbook. Health systems are incurring large losses due to the high cost of contract labor, which grew to 11% of total labor expenses in 2022 from 2% in 2019.9 Furthermore, compensation disparities between temporary and permanent staff and the constant need to educate temporary staff deepen tensions and burnout among permanent staff, prompting them to turn to contract assignments.
It's time to acknowledge that old tools have outlived their usefulness and we need creative solutions to solve the issue at hand and avert future crises.
Recommendations to address the clinician shortage
Our research shows that to address the talent emergency, health systems should fundamentally transform the way they deliver care. This calls for new models for how clinicians work, who they work with, and where they work. While redesigning the work should be at the center, these transformation efforts cannot succeed without ongoing investments in people and rebuilding trust in leadership.
Reimagine care delivery and redesign the work
Truly addressing burnout and improving clinician well-being isn’t easy, according to our interviewed experts, and likely requires a complete care model transformation and job redesign.
Invest in technology to give time back to clinicians
Workflow inefficiencies place a heavy cognitive burden on clinicians. Currently, numerous unnecessary and low-value tasks in clinicians’ day-to-day work take time away from the clinical work. When asked what is one thing that clinicians currently do in their job that has minimal clinical value and could be eliminated, activities to satisfy administrative requirements (32%) and work that could be done by others or automated (20%) were the top two low-value tasks they identified. For physicians, computer-related and insurance-related tasks were the top low-value activities after administrative work. Getting rid of these low-value tasks could offer some quick fixes for optimizing workflows and reducing burnout. For example, the AMA STEPS Forward™ module10 offers a standardized organizational process to identify and eliminate such tasks.11
Given how much time clinicians spend updating EHRs every day, EHR optimization is a critical lever to reduce the burden on clinicians. Organizations can start with EHR analytics to identify tasks that consume large amounts of time across the board and identify areas to reduce clicks and time spent in the EHR. One option is to improve in-basket management. A large medical group eliminated 1.7 million clicks in a year by automatically transferring notifications of admission, discharge, and transfer from physicians' inboxes to case managers. Additionally, use of widescreen monitors made it easier for physicians to keep multiple windows open, further reducing the number of clicks.12
Table of contents
EHRs, in general, have taken much more time than good old paper charts. One example of annoyance are boxes with a maximum number of characters. Sometimes I spend minutes just trying to figure out how to reduce the characters in a medication prescription, comment, or biopsy impression.
I spend so much time trying to pull up the EHR and it closes out after so long of inactivity. If we would have tap badges to sign in and out, it would be much more efficient.
There are other opportunities to use technology to help deliver better care, simplify the tasks, and reduce clinician administrative burden. Our recent research offers some ideas for leveraging automation and other tools to transform physician workflow.
Using technology to automate workflows
- ChristianaCare rolled out a collaborative robot—also known as a “cobot”—to help with nonclinical tasks so nurses can focus on care delivery. Cobots use artificial intelligence to recognize and anticipate when nurses need medications or equipment. Other automated tasks include delivering supplies to patients according to nurses’ orders, fetching medications not kept on the floor, and making rounds to deliver lab samples. This technology can prioritize tasks based on the workload of a unit’s nursing staff to ensure that the busiest nurses receive assistance first.13
- A few organizations are exploring the use of voice activation to automate more of what is done within EHRs, so providers can spend more time with their patients and reduce after-hours time spent on documentation.14
- Our interviewees also look to advanced technologies, like ambient voice technologies and technologies that could help notetaking by capturing doctor/patient conversations, for future solutions.
Specifically for nurses, organizations may consider virtual nursing programs in which virtual nurses work in collaboration with bedside nurses to take care of patients. Virtual nurses help with elements of the job that do not require hands-on care, such as patient education, discharge instructions, or patient monitoring. One benefit of this program is to relieve the work of bedside nurses so they can concentrate on what is most needed at the bedside. Another is to connect bedside nurses with more experienced nurses who can coach and supervise remotely. The goal is to make these opportunities attractive for experienced nurses approaching retirement by giving them flexibility and easing the physical demands of the job (see sidebar, “Can virtual nurses solve the staffing shortage?,” for more information).
Can virtual nurses solve the staffing shortage?
As part of its Nurses Innovate QuickFire Challenge, Johnson & Johnson awarded grant funding for the Virtual Innovative Transformational Nursing Care (VITAL) program. Through this program, virtual nurses operating out of a virtual hospital in Nebraska are connected to 200 on-site nurses at three Community Health Network facilities. These virtual nurses take over duties like collecting medication histories and conducting admissions assessments while also helping to brainstorm with bedside nurses.15
Technology solutions can greatly augment clinicians’ work. When used smartly, technology may even compensate for some of the clinical experience lost as more tenured workers depart. For example, instead of having one experienced in-person charge nurse per unit, interviewed experts expect they can have one virtual charge nurse who can oversee multiple units.
The one thing that we always think about is every time we add new nurses, it dilutes that expertise on the unit; every time we lose an expert nurse, it changes the distribution of what we call “the proficiency index.” The only way that we think that we're going to influence that proficiency index is through new technologies like artificial intelligence.
When considering these technology solutions, it is important that organizations take a human-centered approach, as laid out in our 2021 paper Designing for adoption. This approach can help organizations create more durable and effective solutions that meet both patients’ and clinicians’ needs.
Fundamentally rethink where care is delivered
As more care moves out of hospitals and into outpatient and other alternative sites of care, health systems should be smart about staff allocation and training, and design staff development programs accordingly.
Calls for better staffing were a common refrain in our survey and many of the interviewed experts question the utility of static clinician-to-patient ratios. A better alternative is acuity-based systems that consider the disease burden of the patient panel in allocating resources. Demand forecasting leveraging data, analytics, and cognitive technologies could help make staffing decisions that better match patient needs.
Applying a population health lens, investing in primary care, and catching diseases early can lessen the need for intensive downstream treatment and possibly ease staffing demands in acute care settings. This may involve developing a virtual-first program for healthy and low-acuity patients, risk stratification and identification of patients at risk of chronic illness (e.g., prediabetes), and proactively moving procedures to ambulatory settings, especially for organizations betting on value-based care. Technology can be a key enabler in this transformation, including new diagnostics, sensors, and remote patient monitoring.16
Redesign work teams
The Deloitte 2022 Survey of US Physicians shows that clinicians who use comprehensive care teams find them highly effective (90% say they are effective all or most of the time in in-person settings). And when comprehensive care teams are used, team members largely operate at the top of their license (between 60% and 88% of physicians say different team members operate at the top of their education and skillset most or all the time). Not only are comprehensive care teams useful for developing a more patient-centric, coordinated, and effective care delivery system, but they also help decrease burnout in several ways.
- Creating a culture built on trust and a commitment to team-based care can give employees the confidence to take vacations and remain truly disconnected. We heard it is common for clinicians to work during their time off because they feel the need to be there for their team.
- Employing information technology in novel team-based workflows can help direct messages to the right people, including the extended care teams. As a form of triage, this minimizes the administrative burden for physicians, especially with EHR in-basket messages.
- Bringing more assistive clinical workers to the bedside could also be useful, especially to elevate nurses to the top of their license. For example, one of the interviewed organizations is considering bringing back licensed practical nurses to help bedside nurses with duties like medication administration. Other clinicians can also play a role: Deloitte’s research on the Pharmacist of the future illustrates how pharmacists can provide direct patient care, both in primary and specialty care, under collaborative practice arrangements.
Inject flexibility into jobs
Another untapped opportunity is finding ways to inject flexibility into the jobs. Offering flexible shifts is a good place to start. This gives clinicians (particularly nurses) options that better accommodate their personal needs, whether it’s four-, six-, eight-, or 10-hour shifts. Robust scheduling systems are needed to enable this, and such systems are emerging.17
Everywhere I have worked has been unable to do flexible scheduling despite unanimous requests by staff. Management always says they are open to it, but staffing shortages get in the way.
Job-sharing (splitting a full-time position between two individuals) and mixed work models are other potential solutions to clinician burnout. Mixed work models offer clinicians opportunities to intermix bedside work with other types of work. For instance, clinicians have an option to rotate between inpatient and outpatient, or they can engage in nonclinical work, such as teaching, quality, health informatics, or case management. In this model, the “other” work is formally built into clinicians’ schedule. In the survey, we tested several potential solutions, including flexible shift options and mixed work model (see sidebar, “Clinicians doubt their organizations’ openness to implementing novel programs,” for more information).
Clinicians doubt their organizations’ openness to implementing novel programs
In the survey, we tested four solutions that have the potential to address burnout. We asked respondents about the likelihood of getting these solutions implemented at their organization, their usefulness in addressing burnout, and their practicality for three types of clinicians: registered nurses, licensed practical and vocational nurses, and physicians and advanced practice providers. Of the four solutions, respondents found flexible shift options to be the most useful. For the most part, respondents do not expect to see these solutions implemented.
Invest in your people
In our interviews, we learned that to attract and retain workers, health care organizations should balance extrinsic and intrinsic rewards, recognize cultural, generational, gender, and life stage differences, and address employees’ immediate and long-term professional development needs and interests.
Offer competitive total rewards package
If satisfaction with compensation and benefits is an indicator of how workers feel about their employers’ investments in their people, our survey results point to a glass-half-full scenario: About half of frontline clinicians are satisfied with their compensation (44%) and benefits (51%). And when asked for one piece of advice about how health care administrators can best solve workforce burnout and shortages, more than one-third of clinicians advised offering better compensation and benefits.
Provider organizations should ensure their compensation and benefits packages are competitive. Consider performing analyses to assess how your organization’s compensation and benefits compare to industry and regional benchmarks. In addition to direct industry comparisons, consider compensation and benefits offered by indirect competitors.
Our interviewed experts and surveyed clinicians say that nonmonetary rewards like gratitude days, celebrations, and well-being resources (meditation, yoga, and gym benefits) have a place in the total rewards program.
[Advice to administrators] Allow mothers to be mothers. Offer mothers hours for improved work/life balance. Offer competent affordable childcare.
[Advice to administrators] Improve the workforce benefits. Provide childcare. Don't negotiate contracts over prolonged periods of time!
Create opportunities for career development and mobility
Options for creating opportunities for career advancement and mobility should match employees’ current needs and interests, and anticipate how they might change in the future. One relatively quick fix is promoting the float pool as a developmental avenue. Participating staff benefit from training and opportunities to upskill while the organization benefits by having the flexibility to deploy these individuals across different sites and service lines.
Several respondents spoke about developing relationships with future generations of workers by partnering with nursing and medical schools, universities, and even high schools. These interactions give students insight into what the work could look like and potential opportunities at the organization, and inspire them to come work there. For example, health care organizations could sponsor and support nurses through mentorships, externships, and other opportunities early in their careers or while they are still in school. Programs that help graduates identify the best fit and choose specialization early can help streamline their career path, especially for highly technical specialties such as ICU or OR nursing. One health system that put this program in place five years ago for a difficult-to-fill position (ICU nurse practitioner) saw good success in recruitment for the role.
Career mobility is another area that is lacking at many health systems, according to our survey. Two in five (42%) survey respondents find it difficult to change roles inside their organizations, one-third (33%) say it isn’t possible, and only 25% say such opportunities are available. Having said that, some of our interviewed executives indicated they are beginning to design jobs in a way that allows growth and career progression inside the organization. Examples include training entry-level workers (e.g., medical assistants) to progress to nursing roles. Some respondents’ organizations have created learning journeys that help employees understand the knowledge and skills needed to advance to the next level or to move to an adjacent job function. Other organizations connect team members to career counselors to assist with their career goals. One of the experts described an app that offers employees a way to track their career goals, get insights into internal job opportunities, and connect with employees and mentors with mutual interests and career aspirations.
Provider organizations can also offer residency programs to educate, train, and support new graduate nurses as they transition from academic environments to clinical practice. These programs allow nurses to rotate to different care settings in the first year and gain hands-on clinical experience. This helps increase their capability and confidence, while exposing them to a variety of work and settings that could help them find the best-suited role.
Invest in employee well-being and self-care resources
Clinical workers navigate significant mental and emotional strains daily. The nature of the job often requires workers to deprioritize and sacrifice their own interests and safety. As organizations place emphasis on workers’ well-being and promote self-care, they should normalize the notion that it’s okay to not be okay. In addition to the standard employee assistance program, some organizations we interviewed have stood up comprehensive mental health programs. These programs can have several components, such as an unlimited number of sessions with behavioral health specialists, after-hours availability, and peer support programs. We included an example of a comprehensive mental health program in our concept testing (see sidebar, “Clinicians doubt their organizations’ openness to implementing novel programs,” for more information).
We heard about other helpful initiatives from our interviewed experts. One organization offers its nurses a call line that provides on-demand access to therapists without an appointment. Another conducts short rounds for health care caregivers, a forum for clinicians to come together in a safe setting and talk about challenging topics (e.g., patient deaths) without judgment.
While expanded mental health programs and other well-being initiatives can be immensely valuable, frontline clinicians want to see tangible investments. For instance, vacation policies should be backed by sufficient staff resources to help ensure workers can use all their time off when and how they want to. Especially for nurses, they see a big need to build slack into shift schedules and overall staffing to allow large chunks of time for vacations. Truly disconnected time, time off, and long vacations should be baked into the philosophy and operational processes.
This nurse life of not being able to eat or go to the restroom for 12–13 hours needs to change. Also, a mandatory paid vacation for one or two weeks every couple of months would significantly reduce anxiety and work stress. If rest and mandatory vacations became part of the culture, we would all be much happier and better workers.
Lastly, recruitment and retention efforts should concentrate on all health care professionals. This will help to lessen the burden on nurses who wind up filling the gaps caused by shortages elsewhere.
“We’ve got to focus on the full team, not just the nursing team when it comes to recruitment and retention because anytime there's a drop from a housekeeper all the way to the pharmacist, the nurses are going to take that burden on.”
Restore trust in organizational leadership
For many organizations, an introspective and honest assessment by leadership of its own actions may be in order. How well are you caring for your clinicians?
Trust is an essential element of a healthy work environment18 and plays a crucial part in effective care delivery. Yet, we see an erosion of trust across the health care industry, institutions, and organizations, and among consumers and health workers.19 Our survey findings suggest the damage is severe. Fewer than half (45%) of frontline clinicians trust their organization’s leaders to do what’s right for the patients. Even fewer (23%) trust their leaders to do what’s right for the workers. These two types of trust—to do right by patients and to do right by workers—are highly correlated. Furthermore, the rate of clinician burnout is higher among those who have lost trust in their leadership.
{kind=link}
Health care leaders have a responsibility to rebuild clinicians' trust and restore meaning, value, and purpose in their jobs. This isn’t just the right thing to do, it’s also good for business. Workers at high-trust companies report 50% higher productivity, 76% more engagement, and 40% less burnout compared to workers at low-trust companies, according to a 2016 nationwide study of working adults in the United States.20 We believe transforming care to address clinicians’ pain points can begin to restore the lost trust. Our research highlights several principles that may help organizations achieve this:
Listen, be transparent, and involve frontline workers in decision-making
A true connection between the frontline staff and health care administrators is lacking. Clinicians want to be heard, involved, and kept in the loop. And a diverse and inclusive health care workforce can enrich the discussion by bringing a diversity of experiences and perspectives, creating a sense of belonging, and amplifying voices that traditionally are not heard.21 Nine in 10 of the surveyed clinicians highlighted how important it is for health care organizations to involve frontline staff when developing programs that address workforce burnout and shortages. But only half (54%) said it actually happens, including just 8% who said it happens regularly. The surveyed clinicians said that it’s important for leaders to spend time with their employees. The interviewed experts echoed this advice and highlighted the following actions that their organizations are considering or already have implemented:
- Institute leader rounding, in which leaders are regularly out on the floors, talking to frontline workers in informal settings, observing them as they work, and offering clinicians an opportunity to raise concerns.
- Set up a process that enables clinicians and other frontline workers to share their challenges and help organizations design and implement solutions. Some organizations have established a shared governance council and others have performed hackathons or regularly asked for ideas that are submitted to a formal evaluation process. To build trust, organizations should not only listen to their employees, but also close the loop by keeping employees updated on proposed solutions.
- Conduct employee engagement surveys, compare the results against benchmarks, and use the data to guide future actions. Organizations should use validated survey measures22 and supplement survey data with qualitative input (from town halls, one-on-one conversations, supervisor observations, and advisory councils comprising clinician representatives from all levels) and other workforce analytics data to get a true picture of employee engagement and sentiment.
Stop trying to solve nurses’ problems. Let them frame their problems, let them tell you what the problems are, let them bring forward solutions, let them work across facilities, across units, let them propose solutions, and then support them from the leader’s chair … in developing those solutions and carrying them forward.”
[Advice to administrators] Ask us what would make our work life easier. Ask us or come see what we do daily, don’t just make decisions and implement them without our input.
Restore meaning in a clinician’s job and elevate the humanity of health care
Our respondents highlighted that, in its ideal state, practicing medicine is an incredibly fulfilling and rewarding profession. However, the demands of today’s health care system and the heightened emphasis on the bottom line is sapping clinicians’ joy in caring for patients. Organizations should think of ways to give time and autonomy back to clinicians so they can focus on nurturing patient relationships, a job duty that many clinicians enjoy and derive meaning, value, and purpose from.23 Survey respondents ask for empathy from their leaders, saying they should show them care and respect and treat them as humans rather than numbers.
I feel that one of the big sources of burnout, for me, besides workload and lack of staff, is the lack of respect management has for us as nurses. We are disposable and just a body to fill the spot. It is very discouraging.
Involve frontline clinicians in leadership roles
To help recognize unmet needs and elevate the voice of frontline workers, health care organizations can engage practicing clinicians on committees or cultivate them to join the leadership ranks. Evidence shows that physician-led organizations generally do better in terms of protecting the core values in medicine than nonphysician-led organizations.24 Similarly, interviewed experts spoke of the value nurses add to the C-suite team. Some organizations appoint clinicians to serve at executive levels to ensure clinicians are engaged and involved in decision-making.
Hold leaders accountable for health workers’ well-being
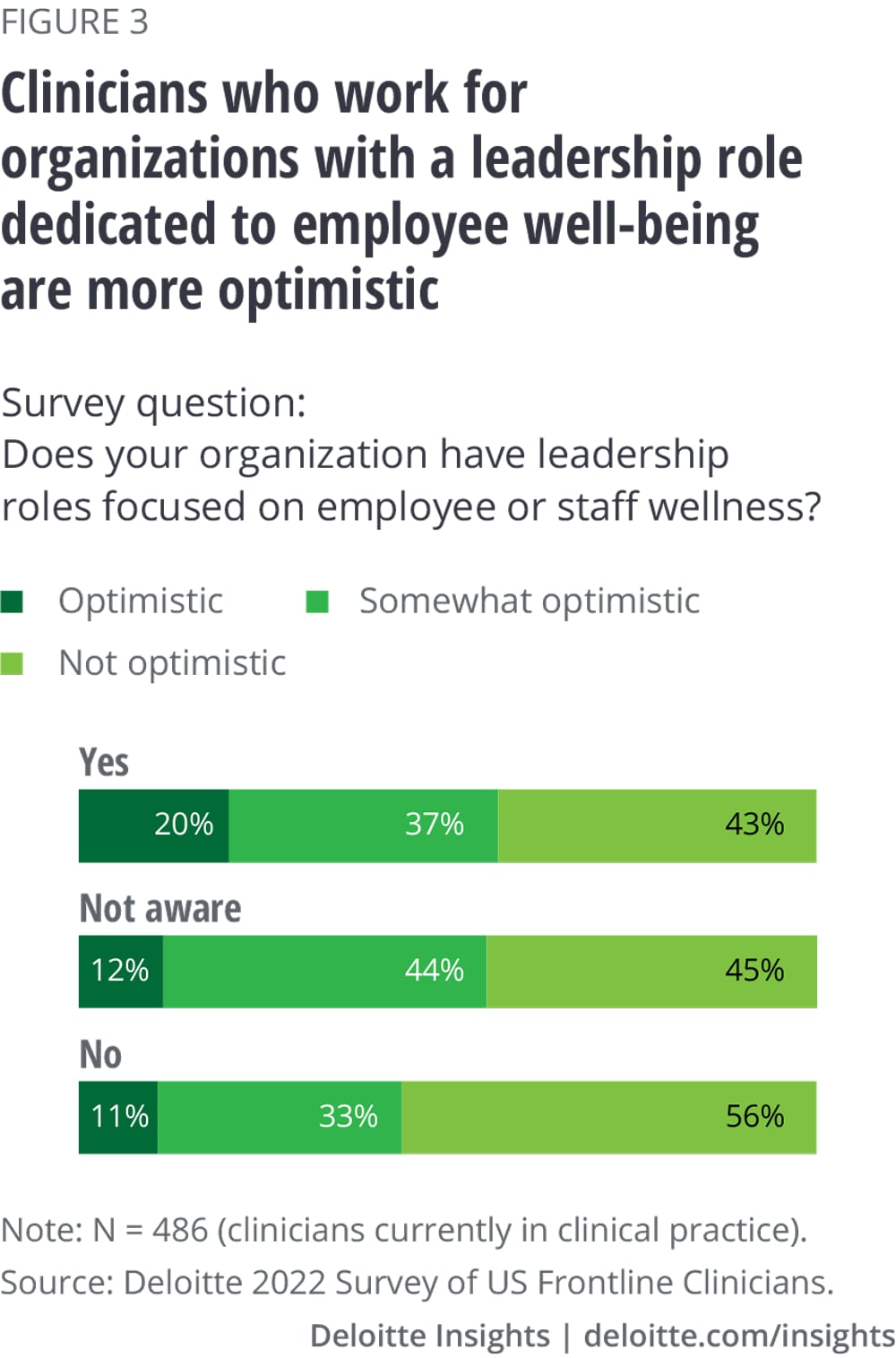
Having supportive leaders who prioritize workers’ well-being can be an important lever to build trust. Some forward-looking organizations have created leadership positions like chief well-being officers to lead efforts dedicated to workers’ well-being. While there are different ways to place these roles in the organizational structure, some recommend that these leaders sit outside of human resources and report directly to top executives. Even though such leadership positions are still uncommon (28% of survey respondents say their organizations have them), when such positions exist, surveyed clinicians report lower levels of burnout.
Interviewed experts stressed the value of providing leadership training and professional development for current and future leaders, at all levels of the organization. One health system enrolls all new leaders into a leadership academy that provides training on soft skills, including sensitivities around cultural and generational differences. Another respondent organization recruits 80% of its leadership roles internally, deliberately building internal leadership pipelines and creating opportunities for clinicians to move into leadership roles. A leadership development academy could also be a venue to proactively identify and cultivate clinicians across the system for the next level of leadership.
In addition, organizations’ leaders should be both accountable and responsible for workers’ well-being. One way to accomplish this is by tying workforce well-being and engagement measures to leader’s performance metrics.
Solving the talent emergency to avert future crises
Frontline clinicians and industry experts are concerned about how clinician shortages have affected care quality and the ability to deliver on health care’s mission. At the same time, they see this as an opportunity to innovate, learn from each other, and create workplaces and a system of care that can enable patients and clinicians to thrive in the Future of HealthTM.
As health care organizations develop strategies to address clinician shortages, they can look to their own clinical staff as a source of innovation and inspiration. Here are a few questions to consider asking to encourage them to engage and share ideas:
- What is one thing that you currently do in your job that has minimal clinical value and could be eliminated?
- If you could break or change one rule in service of a better care experience for patients or staff, what would it be and why?
- What are specific areas or activities in clinician workflows in which technology and tools could be useful?
- Where has technology backfired and what can we learn from that experience?
The mandate to reinvent care delivery comes at a time when margin pressures make it incredibly hard to commit to long-term investments. While hard choices and tradeoffs are unavoidable, perhaps it is possible to design margin improvement programs that optimize costs but also support the goals of improving population health and enhancing the experience of receiving and providing care.
Our findings give us hope: Even though frontline clinicians are largely pessimistic that the industry can find a long-term solution, the outlook is significantly brighter in workplaces that have implemented innovative approaches or when respondents perceive the appetite to do so. We interpret this as a sign that the industry is capable of innovating and can garner the goodwill to commit to long-term strategies to solve the talent emergency and avert future crises.
Appendix 1. About the study
The Deloitte Center for Health Solutions conducted this study to understand the issues of burnout, attrition, and staffing shortages among clinicians, particularly physicians and nurses, and to identify short- and long-term solutions to clinician shortages. Through our research, we explored the innovative initiatives that organizations are implementing to understand what works and what doesn’t, and under what circumstances.
In addition to an extensive literature review, the Deloitte Center for Health Solutions conducted expert interviews and surveyed frontline clinicians (physicians, advanced practice providers, and nurses) to understand the problem and to identify the strategies that health systems are deploying to solve it.
Between April and June 2022, we interviewed 29 industry experts from health care provider organizations, clinician staffing companies, industry groups, and academia. The interview participants represent the following areas of expertise: employee wellness, operations, human resources, strategy, nursing and medical administration, and academic research.
In August 2022, we surveyed 500 frontline clinicians to examine the problem from their perspective and understand their views on the challenge and solutions. The survey included clinicians who currently or recently practiced in acute and ambulatory settings: 250 nurses, 170 physicians, and 80 advanced practice providers.
Appendix 2. Relationship between organizations’ openness to innovation and clinicians’ optimism
{kind=link}
We investigated the relationship between how optimistic workers are that the industry can find a long-term solution to the problem and proxies for health care organizations’ commitment to innovation (figures 3 and 4). Survey participants chose responses from the following list of questions:
- Are you optimistic that the health care industry will find a long-term solution to workforce issues? (“yes,” “no,” or “somewhat”)
- Does your organization have leadership roles focused on employee or staff wellness (e.g., chief wellness officer, chief well-being officer)? (“yes,” “no,” or “not aware”)
- Do you trust your organization's executive leadership to do what's right for the workers? (“most of the time,” “some of the time,” “rarely,” or “never”)
{kind=link}
BY
Maureen Medlock
Ken Abrams
Eileen Radis
Dr. Jay Bhatt
Natasha Elsner
Richa Malhotra
Project team: Gargi Khandelwal, who helped with survey data analysis; Wendy Gerhardt, who provided invaluable guidance on shaping the project and helped edit and review the paper; and Shaun Rangappa and Harish Patel, who provided guidance and reviews of multiple drafts.
The authors would also like to thank Lynne Sterrett, Chandrika Divi, Frankie Reitmeyer, Anubha Bang, Shannon Poynton, Stephanie Lewis, Taylor Cobb, Juli Ozmeral, Vipul Bhatt, Cindy Skirvin, and Diane Sinti for their insights, expertise, and critical feedback on the research. The authors would also like to thank Rebecca Knutsen, Laura DeSimio, Melissa Williams, Zion Bereket, and the many others who contributed to the success of this project.
This study would not have been possible without our research participants who graciously agreed to be interviewed. They were generous with their time and insights. We express our sincere thanks to the following individuals and organizations:
· Shawna Butler, RN, MBA, Nurse Economist; host, SEE YOU NOW podcast; Managing Director, Exponential Medicine
· Tracy Church, Executive Vice President & Chief Administrative Officer, Hartford HealthCare
· Heather Farley, MD, MHCDS, FACEP, Chief Wellness Officer, ChristianaCare
· Joe Greskoviak, Operating Partner, Abundant Venture Partners
· Carrie Hess, Senior Consultant, Integrity Locums
· Tom Jenike, MD, SVP, Chief Well-being Officer, Novant Health
· Stephen K. Klasko, MD MBA, Executive in residence, General Catalyst; Director, Avia Health
· Ajay Kumar, MD, MBA, Executive Vice President, Chief Clinical Officer, Hartford HealthCare
· Eric Langshur, Managing Partner, Abundant Venture Partners; Executive Chairman, AVIA
· Christian Meisner, Senior Vice President & Chief Human Resources Officer, Kaiser Permanente
· Sammie S Mosier, Senior Vice President and Chief Nurse Executive, HCA Healthcare
· Janis M. Orlowski, MD, MACP, Chief Health Care Officer (retired), Association of American Medical Colleges
· Cybele Pacheco, MD, MBA, Population Initiatives, Director of Senior Focused Care, Geisinger
· Amanda Richards, Executive Vice President, Chief Nursing Officer, Hartford HealthCare
· Jonathan Ripp, MD, MPH, Senior Associate Dean for Well-Being and Resilience and Chief Wellness Officer, Icahn School of Medicine at Mount Sinai
· Tina Shah, MD, MPH, Principal, TNT Health Enterprises LLC
· Mark Smith, Vice President, Workforce Strategy & Analytics, Providence
· Colin P. West, Physician, Mayo Clinic
We thank our other respondents whose permission to be named in this report was not received in time for this publication.
Cover image by: Sonya Vasilieff.