Why doing many of the right things still may not be enough to transform care delivery
In a new care delivery transformation index, surveyed health systems scored themselves 2.7 out of 5 on the ability to turn transformation efforts into scaled, AI-enabled operations
Most health system leaders know where care delivery should go. In a new survey by the Scottsdale Institute and Deloitte, 100% of respondents said care delivery transformation is either a top enterprise priority (63%) or very important (37%). Many have already made the case for change, aligned leadership, launched pilots, and begun deploying artificial intelligence. By most measures, they’re taking many of the expected early steps.
Yet they reported that turning that momentum into sustained operational change remains difficult—and slow.
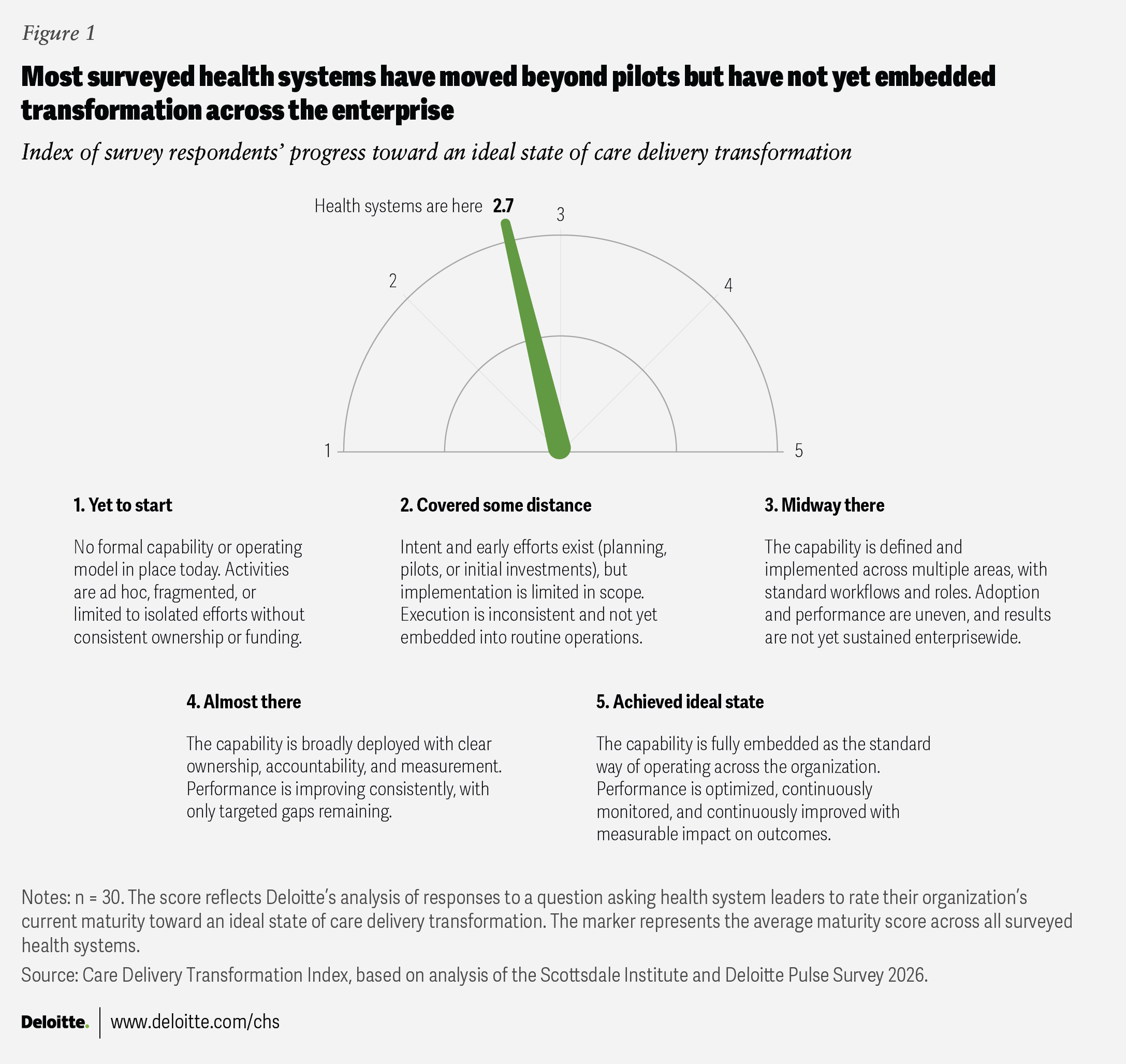
In our new care delivery transformation index, health systems give themselves an average score of 2.7 out of 5 on their ability to scale care delivery transformation (figure 1). This places organizations, on average, beyond planning and pilots but still short of transformation at scale (see methodology). For this study, care delivery transformation means redesigning care models—across workflows, workforce, sites of care, technology, and partnerships—to deliver more proactive, personalized, and connected care around the person rather than the facility.
Based on a survey of 30 health system executives, including CEOs, chief information officers, chief financial officers, and clinical leaders, the research offers insights into where care delivery transformation stands today and what may be needed to scale it over the next three years.
The conventional narrative is that health systems remain constrained by limited capital, immature technologies, or workforce resistance to change.1 Those pressures are real. But our survey points to a more nuanced story: Many organizations that feel stuck may not lack resources or resolve. They have invested in data infrastructure, secured executive sponsorship, and moved AI from experimentation into targeted operations. What many organizations still haven’t done is embed transformation into the enterprise’s default operating model.
Transformation delays may stem from limited capacity to execute at scale, not a lack of foresight
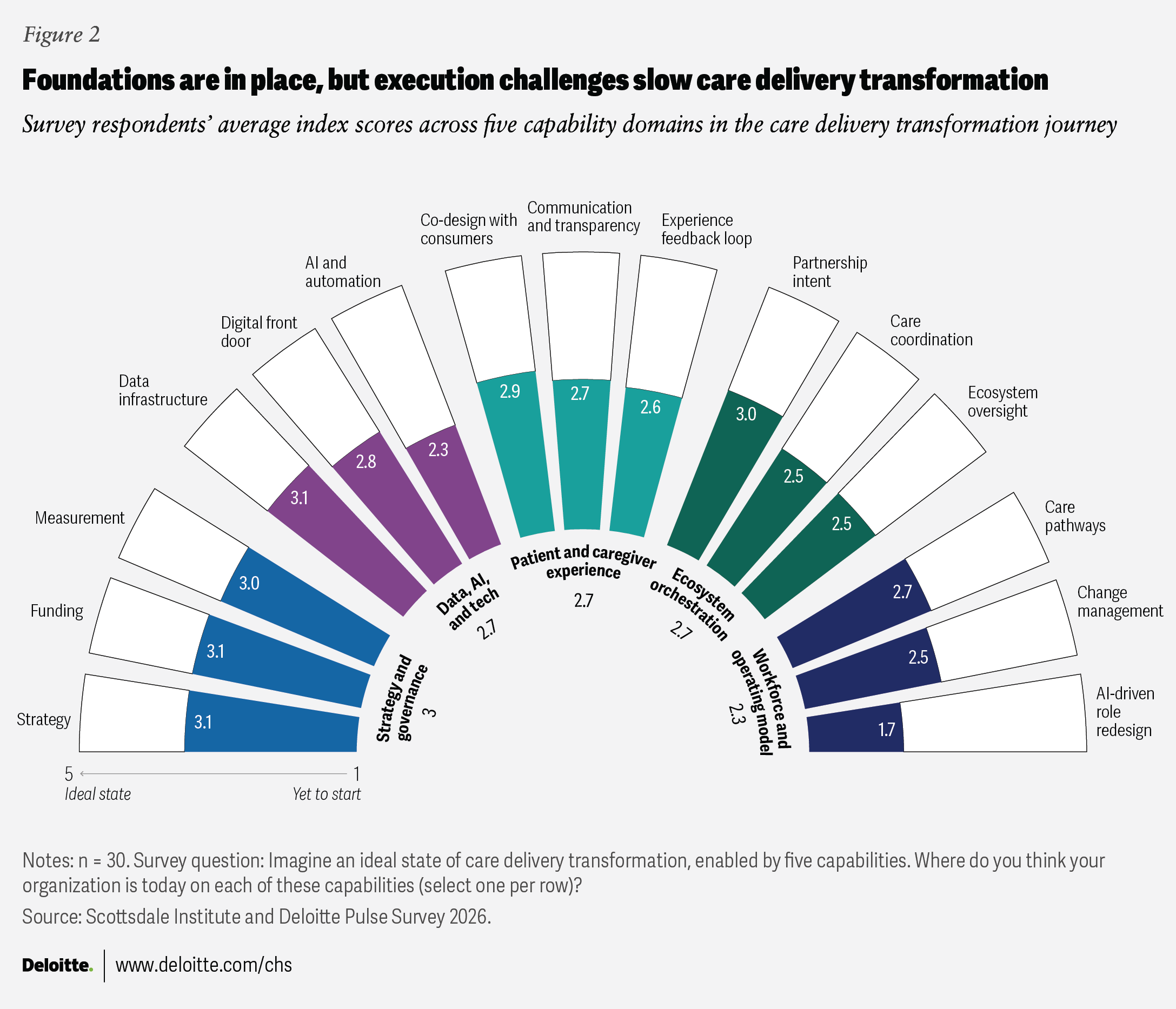
In our survey, health systems scored themselves higher on foundational transformation capabilities (figure 2). Stronger positioning in strategy, data infrastructure, funding, measurement, and partnerships (including ecosystem and growth-oriented collaborations), may suggest meaningful investment and sustained executive attention.2 In contrast, the lowest scores appeared in areas where enterprise change becomes most operationally complex and disruptive.
AI-driven role redesign scored lowest, at 1.7, possibly reflecting a common pattern: Health systems often deploy AI as a point solution rather than embedding it into end-to-end workflows.3 AI and automation, care coordination, and ecosystem oversight also scored relatively low, at or just below 2.5. Taken together, the results reflect real progress in strategy, infrastructure, and leadership alignment, but also reveal how much work remains to translate that foundation into enterprisewide operating change.
The hardest work generally begins after the strategy is set and pilots show promise. Scaling involves different capabilities than planning: deciding which initiatives deserve enterprise backing and which should be discontinued; redesigning work rather than layering tools onto existing workflows; standardizing processes where variation no longer adds value; and establishing accountability mechanisms that endure beyond the launch phase.
These insights suggest that health systems may be entering a more demanding stage of transformation, one in which success could depend on whether an organization can embed new workforce models, routines, and priorities into day-to-day operations. One survey participant, a chief value officer, noted in an open-ended response,
“The next three years will determine whether health systems become more resilient, effective, and sustainable, or continue to bear increasing pressure without the tools to succeed.”
Three execution gaps leaders recognize but are still working to close
The survey highlights three execution gaps that appear across surveyed health systems of different sizes, structures, and markets. Overall, leaders report that they see these gaps clearly, and many have begun to address them. The data suggests that awareness may not be the bottleneck. A challenge is building the organizational muscle to act consistently and at scale on what leadership already knows.
Determining which transformative models to scale
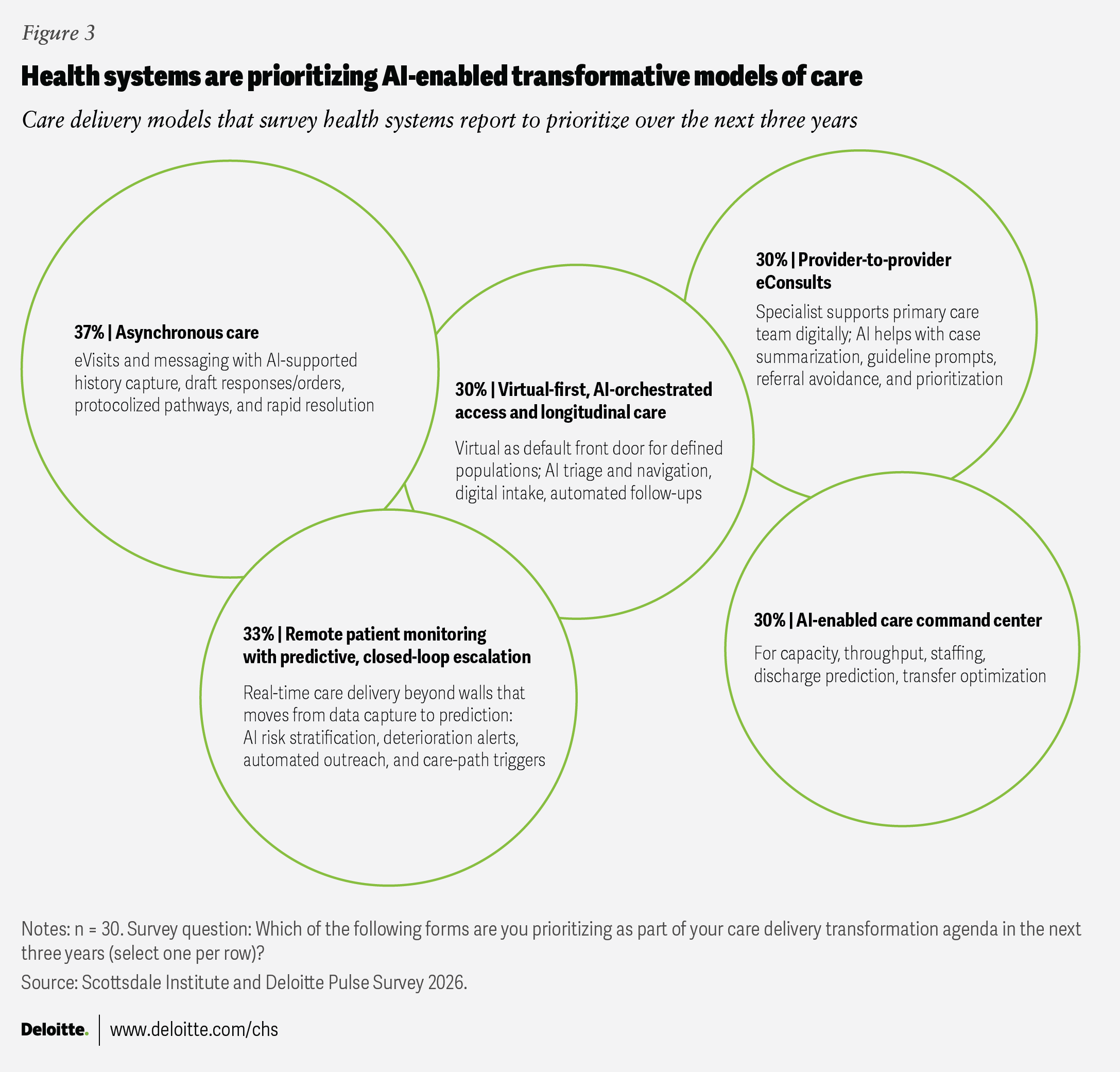
Thirty percent of surveyed leaders said their organizations are piloting four or more care models simultaneously, including post-acute coordination, command centers, virtual-first access, and remote patient monitoring.
The findings suggest that health systems are actively testing a range of innovation pathways. But running multiple plausible pilots in parallel also can increase the pressure on leaders to make tough enterprise decisions. More than half of respondents (57%) said the clearest accelerator of progress in the 12 months following the March 2026 survey would be clear leadership decisions about what to scale and what to stop.
To sustain momentum, organizations may need to move faster to increase investments of time, capital, and leadership attention in models that show the strongest potential for measurable value and enterprise adoption, while exiting those that don’t (figure 3).
The experience of early movers offers useful signals. UC San Diego Health launched a virtual transition-of-care clinic that provides rapid post-discharge follow-up, medication reconciliation, and specialty care navigation for moderate- to high-risk patients. According to the organization, the program reported a 30-day hospital readmission rate of 14.9%, compared with a 20.1% average in the benchmark cohort based on a three-year study.4 The example suggests that a virtual-first model can extend care delivery beyond hospital walls and support more continuous care management when it is resourced and operated as part of the core model.
Houston Methodist offers a similar example of how predictive monitoring can move remote patient monitoring beyond data collection and toward earlier escalation and tighter integration with operational response pathways. The organization implemented a model that paired continuous wearable surveillance with enhanced rapid-response workflows to identify deterioration earlier in hospitalized patients. A clinical study of the model showed lower severity of illness at ICU transfer, shorter total length of stay, and lower in-hospital mortality.5
Together, these examples suggest that value can become clearer when transformative models are integrated into routine operations rather than left in prolonged testing.
Survey respondents also pointed to additional models for future exploration, including virtual safety monitoring, smart-room technologies, AI-enabled refill workflows, tech-enabled care models for uninsured populations, and AI-supported specialty access. These priorities align closely with persistent pressures around access, cost, and workforce capacity.6 However, organizations can identify potentially valuable innovations, yet make little progress if those intentions remain sidelined with pilots. The findings suggest progress is more likely to accelerate when leaders make deliberate choices about which capabilities to operationalize across workflows and day-to-day decision-making.7
Training the workforce without redesigning roles can create transformation drag
The gap between change management capability (2.5) and AI-driven role redesign (1.7) suggests that many health systems may be equipping staff to use new tools before fully rethinking how work should be organized around them. That sequence can cause friction: Technology layered onto legacy workflows can add complexity without delivering the full benefits of transformation. One chief medical officer we surveyed notes in an open-ended response:
“Care teams must be redesigned so clinicians can work at the top of their license, supported by technology. Transformation isn’t optional—it’s necessary to retain talent and preserve access.”
Staffing shortages and rising labor costs reinforce the same point.8 Lasting transformation is more likely to come from redesigned roles, team-based care models, and operating structures aligned with future AI-enabled care workflows, rather than from introducing new tools into siloed ways of working.
CommonSpirit Health’s virtually integrated care model is one example of this approach. The model integrates a virtual registered nurse into the unit-based care team to assume documentation, coordination, education, and monitoring tasks that don’t require hands-on bedside care, allowing bedside nurses to focus more on direct patient care and mentorship. According to the health system, across 1,075 beds, the model supported 808,200 virtual visits in 2025 and was associated with a 43% reduction in voluntary turnover among first-year registered nurses and a 21% decline in emergency department hold hours. The organization also reported improvements in patient experience and infection outcomes.9
Partnership ambition outpaces orchestration
The index reflects partnership intent at 3, while execution in care coordination and ecosystem oversight lagged at 2.5 (figure 2). That gap suggests that many organizations are still early in enabling their networks to operate as integrated systems. Health systems are increasingly pursuing care quality and care coordination goals through partnerships, joint ventures, clinically integrated networks, and affiliations.10 At the same time, data and workflow integration remain central challenges: In 2023, 70% of US hospitals engaged in some form of interoperable exchange. However, the integration and routine use of external clinical information remained uneven, especially among lower-resourced organizations and nonhospital partners such as post-acute and behavioral health providers.11
To help them succeed in a market defined by value-based care, longitudinal management, and growing demand for seamless post-acute and community-based support, health systems may need to translate partnership intent into operational coordination by aligning workflows, processes, and patient management across organizations. One chief digital and innovation officer notes in an open-ended survey response:
“Nobody has figured out efficient and effective care coordination. To lower the cost of health care in our country, we have to get this right.”
Intermountain Health’s partnership with UCHealth offers one example. In Colorado, the organizations launched a partnership to build a clinically integrated network bringing together 700 primary care physicians and hundreds of clinics and hospitals, with the stated goal of improving care coordination, delivering higher-quality care at lower cost, and introducing a new insurance option in the market. The partnership was designed to support more than 300,000 residents, illustrating one pathway for translating partnership strategy into a more scalable, value-based model.12
Three moves that can accelerate care delivery transformation
The gaps described above appear to be primarily operational rather than structural, which suggests they can be narrowed through the appropriate organizational choices. Our survey findings point to three actions that could help accelerate transformation:
Build governance to scale. Respondents identified decisive leadership regarding what to scale and what to stop, along with dedicated transformation governance and execution capacity, as top accelerators in the 12 months following our March 2026 survey. Faster-moving organizations appear to be building dedicated governance and execution capacity, rather than relying only on periodic oversight. In practice, this could entail building enterprise governance across business strategy, digital, AI, and data functions so that transformation efforts are aligned, decision-making is streamlined, and innovations are either integrated into daily operations or shut down before they become a financial drag.
Shift from buy-in to co-ownership. Forty percent of surveyed executives identified stronger clinician co-ownership and accountability as a top accelerator. This tends to move the conversation beyond clinician buy-in, which often assumes the core design work has already been done. Co-ownership means clinical leaders help determine where redesign should occur, what trade-offs are acceptable, and how new models should be assessed. Involving consumers in the codesign of pathways, communications, and tools can also improve patient and caregiver experience. An earlier Deloitte–Scottsdale Institute study underscores why this matters: End-user involvement is often associated with stronger transformation outcomes, yet clinician engagement still remains uneven across many organizations.
Measure the value that matters. One-third of respondents selected clearly defined key performance indicators and periodic measurement as a top accelerator. This aligns with another recent Deloitte–Scottsdale Institute article, which found that health systems often default to narrow implementation and savings metrics even when broader sources of value, such as consumer experience, workforce productivity, brand reputation, and opportunity cost, matter just as much. To help sustain momentum, leaders should not only measure these outcomes but also communicate and reinforce them consistently through metrics that signal what success looks like. Health systems may struggle to sustain transformation when scorecards emphasize only near-term cost savings or implementation milestones rather than the outcomes leaders say they want.
The definition of transformation may be shifting, and that could be an advantage
When asked what would prove care delivery transformation was worthwhile three years from now, health system leaders were relatively clear. Sixty-three percent pointed to lower cost of care, and 57% said better clinical outcomes. Far fewer prioritized financial growth, at 23%.
Those responses suggest that success may be moving away from growth alone and toward something fundamental: care that costs less, works better, and is more sustainable to deliver.
That clarity could become a competitive advantage. When leadership teams focus on affordability, outcomes, access, and workforce sustainability, they can make sharper decisions about where to invest, what to stop, how to redesign roles, and how to measure progress. It can also help move the conversation away from the idea that organizations need to choose between financial discipline and transformation.
The transformation index suggests that the organizations that may be best positioned to advance are not necessarily those with the most resources or the most sophisticated technology. They may be the ones most able to translate what they already know into operating reality across workflows, roles, and day-to-day decisions. That translation is difficult work, but it’s often what determines whether transformation endures beyond the initial launch.
Methodology
The Scottsdale Institute and the Deloitte Center for Health Solutions surveyed 30 senior technology, strategy, and clinical leaders from medium-sized and large US health systems and academic medical centers between February and March 2026 to assess organizational progress in care delivery transformation.
For this study, care delivery transformation is defined as a deliberate reset of care models (including workflows, workforce, sites of care, technology, and partnerships) so that care becomes more proactive, personalized, and connected across the continuum from prevention through long-term support. In this definition, care is organized around the person rather than the facility, with the goal of improving outcomes, access, experience, and cost.
To benchmark transformation maturity, the study introduced the care delivery transformation index. Respondents rated their organizations across 15 capabilities currently spanning five categories: strategy and governance; workforce and operating model; data, AI, and technology; patient and caregiver experience; and ecosystem orchestration. For each capability, respondents used a five-point maturity scale ranging from “yet to start” (1) to “achieved ideal state” (5).
Capability scores were calculated as average scores based on the distribution of responses for each item. Category scores represent the average of the capability scores within each category. The overall care delivery transformation index position represents the average of the five category scores, producing a composite measure of organizational maturity.
Continue the conversation
Meet the industry leaders
Bill Fera
Janet Guptill
by
Christy Lemak
Bill Fera
Anwesha Dutta
Dr. Jay Bhatt
Maulesh Shukla
Madhushree Wagh
The authors would like to thank Nivedha Subburaman for her significant contributions to the research design, analysis of the key findings, and writing of key sections of the paper, and Alluri Rohith Reddy for hosting the survey and assisting with data queries.
The authors would like to thank Janet Guptill, John Hendricks, and Jennifer Gadney from the Scottsdale Institute for their insights, expertise, and input on the research.
The authors would like to thank Alicia Janisch and Melissa Williams from Deloitte for their work supporting the Scottsdale Institute and Deloitte relationship. The authors would also like to thank Rebecca Knutsen for her significant contributions to editing and structuring the paper. Additional thanks go to Christina Giambrone, Wendy Gerhardt, Shyamili M, Jared Johnson, and the many others who contributed to the project.
This study would not have been possible without the participants who graciously agreed to take part in the survey and interviews. The authors wish to thank them for being generous with their time and insights.
Editorial (including production and copyediting): Rebecca Knutsen, Shyamili M, Cintia Cheong, and Anu Augustine
Design: Meena Sonar, Natalie Pfaff, and Harry Wedel
Cover image by: Meena Sonar
Knowledge services: Vanapalli Viswa Teja
Visit the Deloitte Center for Health Solutions
Access more insights for the hospital, health system and provider, pharmaceutical manufacturer, health plan and payer, medtech, and health tech organization sectors.