A ‘whole health’ approach to health care transformation
Rewiring the US health care system to create a more efficient, affordable, and effective ecosystem that promotes wellness and extends the health span for all Americans
Key takeaways
- The United States outspends peer nations on health care but has some of the poorest health outcomes for its dollar.1 Life expectancy has not returned to pre-pandemic levels, maternal and infant mortality ratings are low, and chronic disease burden remains high.2
- Differences in disease burden are at the heart of poor health rankings. A person’s zip code can have a greater influence on health outcomes and health span than visits to the doctor.3
- A whole health approach can improve the health of the US population and save lives—and may save costs. By investing in drivers of health, realizing the value of prevention, and leveraging substantial scientific breakthroughs to optimize prevention and wellness, we can improve health outcomes and lead to healthier and longer lives as well as save lives.
- Embracing systems change is crucial to success. Shifting health trajectories requires shifting not just how we think about health but how the health system is designed and connected. Government can partner with industry to build bridges across the health care ecosystem through systems change, paving the way toward an interconnected, navigable health system focused on longevity and optimized wellness.
Imagine a future in which the typical American life span is extended by 12 years, with nearly 90% of those years lived in good health.4 This not only means a longer life span for the average American but also a better health span, granting Americans almost 20 additional healthy years. Remarkably, achieving extended and healthier lives doesn’t necessarily require additional health care spending. It could mean spending less.5
The current US health system is set up to provide episodic and fragmented care. Five years ago, Deloitte outlined its vision for the future of health, predicting a monumental shift from a reactive “sick-care” system to a proactive “well-care” system. In this model, consumers and their care teams will focus on early detection and prevention of illness rather than merely treating disease. A Deloitte US actuarial analysis projects that, without these changes, health spending could triple to nearly $12 trillion by 2040. But our model also suggests that transitioning to Deloitte’s vision for the future of health could limit spending to $8.3 trillion.6
Table of Contents
- Expenditure-outcome disconnect
- Transforming health care ecosystem
- Preparing for change
Turning this vision into reality requires a pivot away from the traditional understanding of health as being solely about treating ailments, to embracing a holistic, well-being-centered approach. It’s about integrating prevention, mental, spiritual, emotional, and financial health, and social factors alongside physical health to create a future where everyone can live longer and healthier lives. For this transformation to materialize, it is crucial that all relevant stakeholders take on the role of change agents. These stakeholders include government agencies, health care organizations, life sciences companies, insurance companies, pharmaceutical firms, technology providers, patient advocacy groups, research institutions, and the public.
The “whole health” approach is an important component of Deloitte’s vision for the future of health. Whole health emphasizes improving or sustaining the health of the individual rather than merely treating the individual’s diseases and illnesses. Whole health efforts, which focus on improving living conditions and investing in lifelong health development, can help elevate the health status of entire populations. To achieve this, an increasing number of health care organizations and government agencies are recognizing the need to consider the drivers of health or factors such as lifestyle, nutrition, income level, education, and environmental conditions that disproportionately affect health outcomes.
Creating whole health by intention and by design calls for various entities to forge robust alliances and a holistic and coordinated strategy for health and well-being that can improve health opportunities and outcomes for all. This potential paradigm shift mirrors what Americans want from a health system: one that not only promotes wellness but also empowers them to participate in and make decisions about their care.7
The US health care system needs an overhaul to help address the rising costs, quality gaps, and health differences that impact many Americans. However, despite its shortcomings, the existing system is also brimming with opportunities for innovation and collaboration. Government partnerships with health care stakeholders could prove instrumental in this transformation by prioritizing health and wellness, employing strategies for systems change, investing in value-based care, and modernizing data infrastructures.
What’s now: A persistent disconnect between expenditures and outcomes
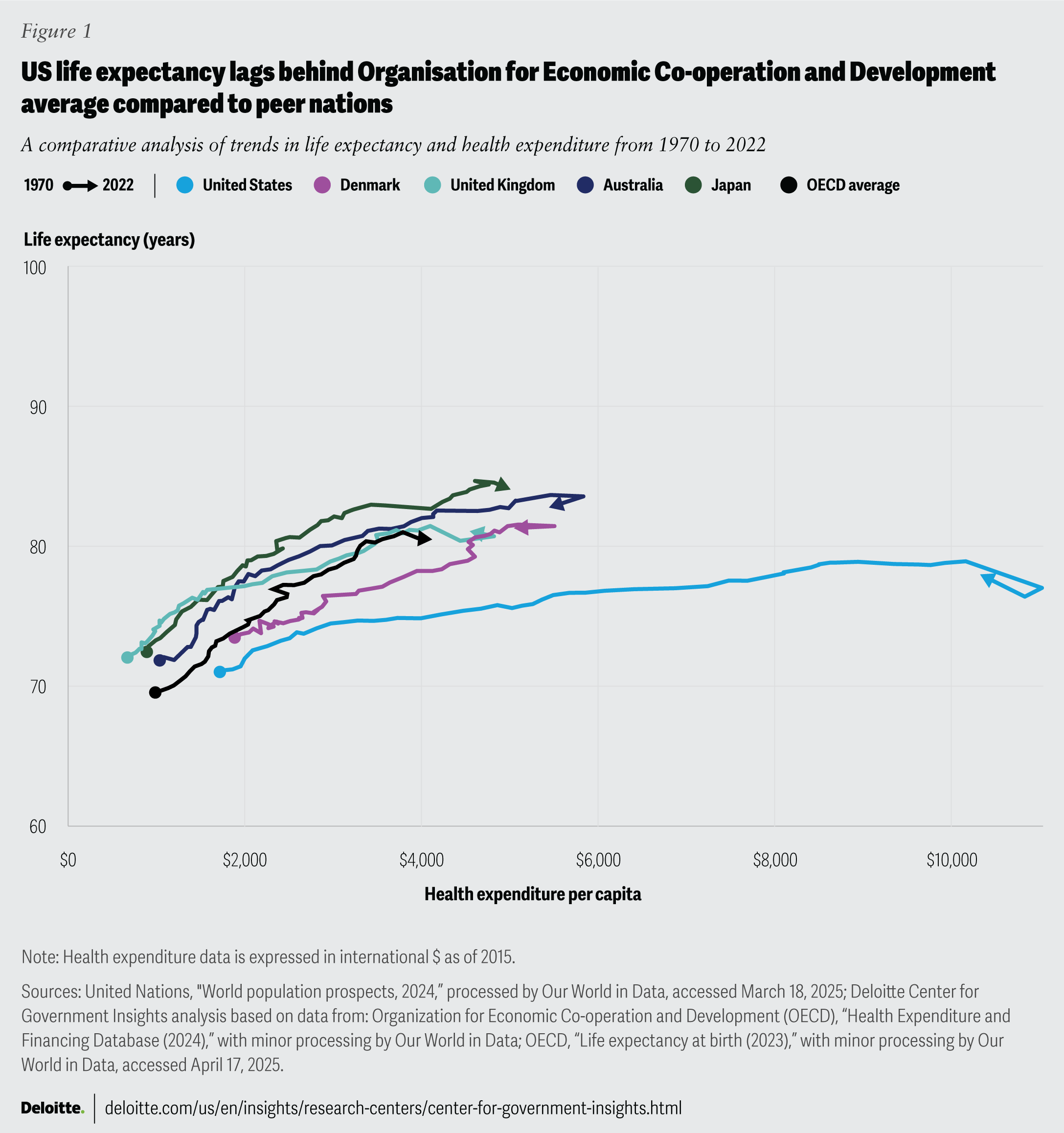
The US government spends more on health care than any other country: In 2021 alone, the United States spent 17.8% of its GDP on health care, nearly twice as much as Germany and around four times more than South Korea.8 Yet this considerable spending does not translate into better health outcomes: The United States also ranks poorly on many health indicators, such as life expectancy, infant mortality, and chronic disease burden.9 In 2022, life expectancy at birth, a critical measure of a nation’s overall health, was 76.4 years,10 which is significantly lower than the OECD average of 80.3 years (figure 1).11
The US government spends more on health care than any other country: In 2021 alone, the United States spent 17.8% of its GDP on health care – almost double Germany's and quadruple South Korea's spending.
{kind=link}
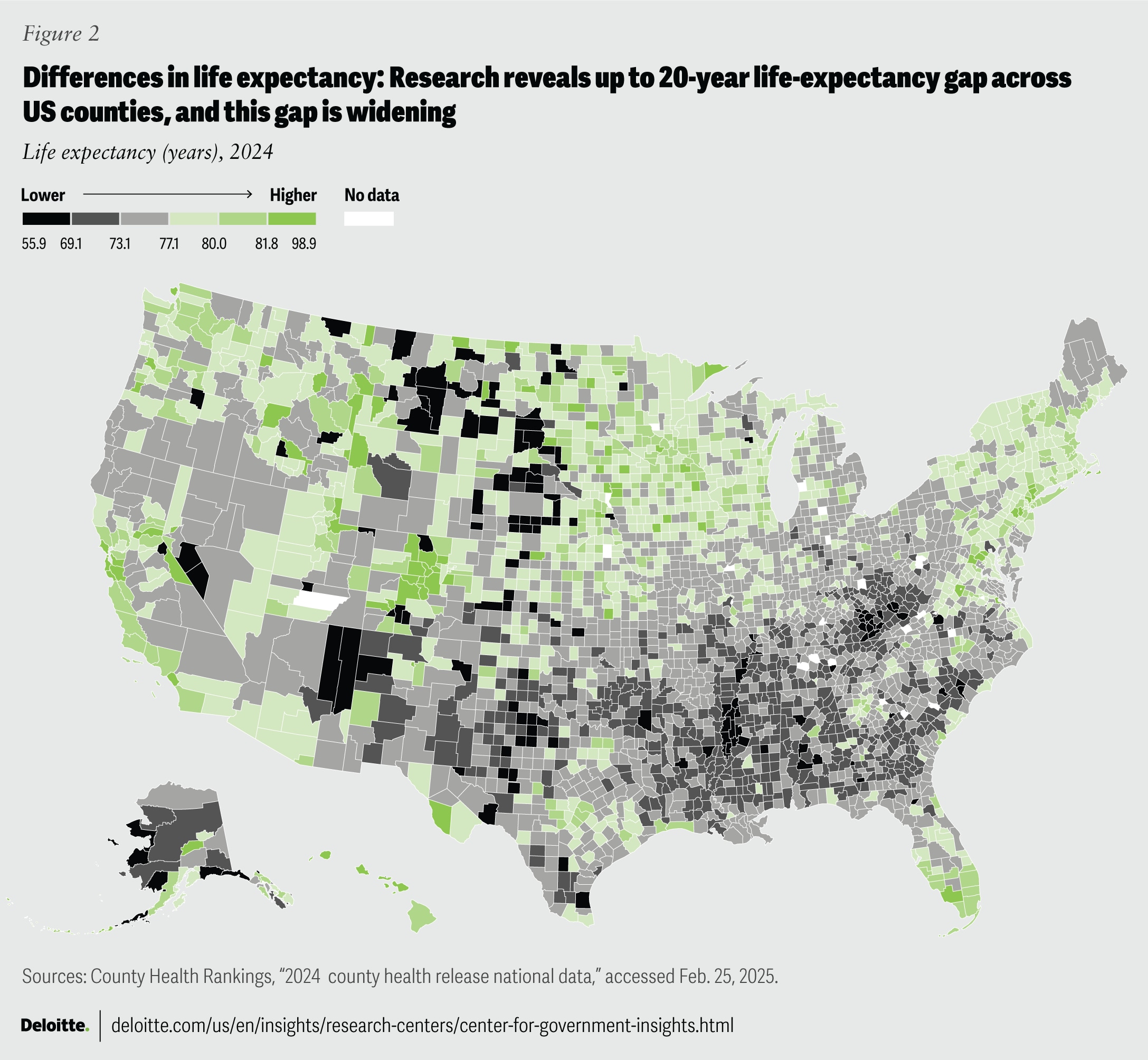
Life expectancy across the United States varies considerably based on the drivers of health, such as the conditions where people live. One in five Americans live in neighborhoods with high crime rates, pollution, unstable housing, limited employment opportunities, and lack of access to nutritious food.12 One study found up to a 20-year difference in longevity by county, and that gap has been widening (figure 2).13
{kind=link}
The health sector has long acknowledged the need for holistic, multisectoral, and preventive approaches to health and well-being,14 but progress has been slow and uneven. In contrast, investments in artificial intelligence and biomedical innovation in the health sector are growing. A study conducted in March 2024 found that 79% of health care organizations were using AI technology.15 In 2022, the National Institutes of Health dedicated an estimated $130 million over four years to the development of new biomedical and behavioral AI-based data sets to prevent disease and identify factors linked to better health.16 Already researchers have created data sets to study priority research areas like type 2 diabetes disease progression, and the use of patient vocal patterns to diagnose diseases like cancer.17 With new AI developments, it will be important for industry to solve for the right problems. Equally important, government and industry can collaboratively design protective measures to support the responsible and secure use of these technologies.18
Despite numerous efforts in the last few decades to reform the health system, the United States continues to lean on a fee-for-service model that incentivizes volume over value, emphasizing treatment over prevention.19 Moreover, the health system remains fragmented and siloed, making it difficult for patients to navigate it to access the care needed. This also complicates the process for providers to coordinate and integrate services across the continuum of care.20
What’s next: The role of government and industry leaders in driving transformative change in the health ecosystem
Government leaders and industry partners can catalyze the shift in health and well-being by using their unique position and influence to help drive systems change across the health ecosystem. Leaders can tailor strategies and interventions to the specific needs and assets of various communities and populations by engaging with stakeholders, leveraging data and evidence, and fostering innovation and learning. However, this holistic view can only be realized through collaboration across the ecosystem.
To create a more integrated and resilient health system, leaders need to look beyond the traditional boundaries of health care. A vision for the future is one that is more connected, focused on prevention, and designed to meet individual needs. This will require a financial model focused on improving the health of all Americans, in addition to treating disease. Here are a few ways that leaders can promote whole health.
- Adopt an ecosystem approach. Government and industry leaders can foster a health system that is more responsive and adaptive to the needs of people and communities by taking an ecosystem approach to coordinate efforts across different agencies and domains. This strategy involves aligning the goals, policies, and actions of different government agencies and levels along with nongovernmental partners and communities.
The US government has already taken steps to apply a whole-of-government approach to well-being. The President’s new Make America Healthy Again Commission adopts a whole-of-government approach to tackle critical health challenges faced by Americans, with the intention of reducing chronic disease rates. The initiative will work to make US food the healthiest, most abundant, and affordable in the world, among other aims. The commission also focuses on ending chronic diseases in children.21 It is composed of leaders across the federal government, including health, agriculture, housing, education, environment, and others. The strategy will emphasize new approaches to health promotion, a greater understanding of influences on child health like technology use and environment, and transparency in health research.22
Another example is the Healthy People 2030 initiative—a national agenda for improving the health of all Americans led by the Health and Human Services’ Office of Disease Prevention and Health Promotion.23 The 10-year initiative sets objectives for whole population health improvement, such as increasing US health literacy. It also provides data and tools to help public health organizations monitor progress and implement evidence-based interventions for health issues ranging from chronic diseases to injuries and violence and even encompasses mental and emotional well-being.
Leaders can harness an ecosystem strategy to target health issues with substantial societal costs that often lack sufficient investment, like tackling the underlying factors of poor health and health differences which have massive economic costs.24 According to a Deloitte 2022 analysis, gaps in health opportunity account for approximately $320 billion in annual health care spending, signaling an unsustainable crisis for the industry. If left unaddressed, this figure could grow to $1 trillion or more by 2040.25 Another Deloitte analysis estimates that differences in mental health outcomes will lead to excess costs of $477.5 billion in 2024, escalating to over $1.3 trillion by 2040, with a cumulative societal cost nearing $14 trillion, or about $42,000 per person in the United States.26 These rising costs don’t just strain the health care system, but also cut into Americans’ economic and social potential. Addressing affordability and differences in outcomes can advance the full potential of health for everyone in our nation.
An ecosystem approach can play a pivotal role in addressing challenges facing certain groups. Nonprofit health system Saint Alphonsus took a bold step to help alleviate rural health challenges in Idaho.27 After identifying housing affordability as a top concern in the state, Saint Alphonsus partnered with a local nonprofit that united 10 ecosystem partners in finance, health care, and philanthropy to fund a community land trust.28 The trust, which began in Boise and is now expanding to rural areas, funded the creation of 25 homes that will remain affordable even as housing prices rise.29 It demonstrates the power and promise of ecosystem stakeholders inspiring each other to make health more accessible, even beyond the point of health care delivery.
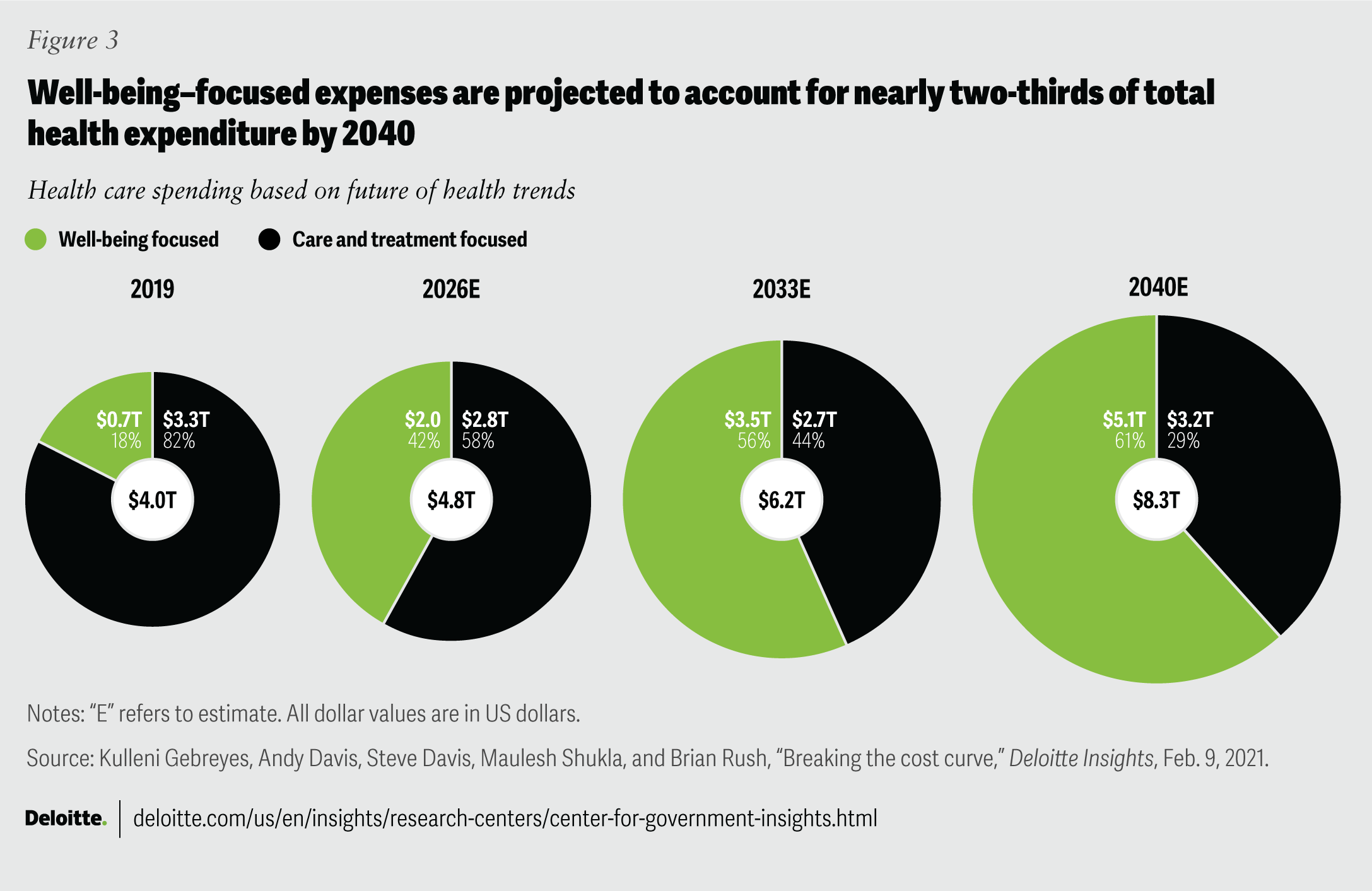
There’s a financial upside, too. Future health spending will likely need to shift toward platform ecosystems that connect health data across institutions, and user-friendly apps for healthy living. More health care organizations will likely need to commit to tackling drivers of health. By 2033, these well-being-focused expenses are expected to surpass treatment costs. By 2040, the expenses could constitute nearly two-thirds of total health spending, making up 11.3% of the GDP, with the rest going toward treatments and diagnostics (figure 3).30
Expanding horizons: To create a more integrated and resilient health system, leaders need to look beyond the traditional boundaries of health care.
{kind=link}
- Usher in place-based change. One way to build bridges across the health ecosystem is to design and implement targeted approaches that respond to the needs and preferences of different communities. This model acknowledges that health organizations alone cannot address the complex and interrelated needs of individuals and families. Health organizations should instead look for opportunities to partner with community-based organizations, businesses, and others—including area residents—to identify needs and provide the right resources, such as improved access to education, food, housing, and employment.
Place-based change initiatives aim to improve the health and well-being of people living in a defined geographic area by addressing the social and environmental factors that affect health. For example, the Massachusetts Housing Investment Corporation and Conservation Law Foundation manage a collaborative fund with financial investors, hospitals, and insurers aimed at building high-quality housing in urban areas around Boston to help drive health improvements.31 The key to success has been a community-led continuous research process. Community members collect data and use it to assess quality and share outcomes with investors, partners, and the wider community. Improving community health is a collective responsibility and effort that requires the active involvement of all stakeholders to achieve lasting change.32
Another example is the Magnolia Community Initiative, a social innovation network that includes more than 80 partners (for example, social services, faith-based organizations, universities, public services, financial services, schools, health care providers, and community residents). The network, which has been in operation since 2008, has a shared goal of improving the well-being of children and families living in a low-income catchment area of Los Angeles. The Magnolia Community Initiative serves 35,000 children within a 500-block radius who have faced poverty, low graduation rates, and poor nutrition, and many are not prepared for kindergarten.33 To ease the burden of multiple trips to different service providers and repetitive, cumbersome paperwork, the network offers a co-location of health, education, and social service providers, and a single, streamlined interface to access them. Magnolia Community Initiative has also created a cross-sector referral and follow-up system to support families’ access to resources outside of the community hub.
Launched by the United Way of Southern Maine, the Thrive2027 initiative employs a community dashboard to track collective progress toward regional health goals in Cumberland County: providing children with a solid foundation, enabling residents to thrive rather than just survive, and enhancing the collective longevity and quality of life. The initiative has built a wide network of over 302 partners across government, schools, nonprofits, businesses, and philanthropy. As a result of the efforts through this initiative, there have been improvements on multiple fronts: Food insecurity has fallen from 16.6% to 11.2% between 2017 and 2021; and there has been an increase in the percentage of available high-quality early childhood programs from 14.1% in 2019 to 19.1% in 2023.34
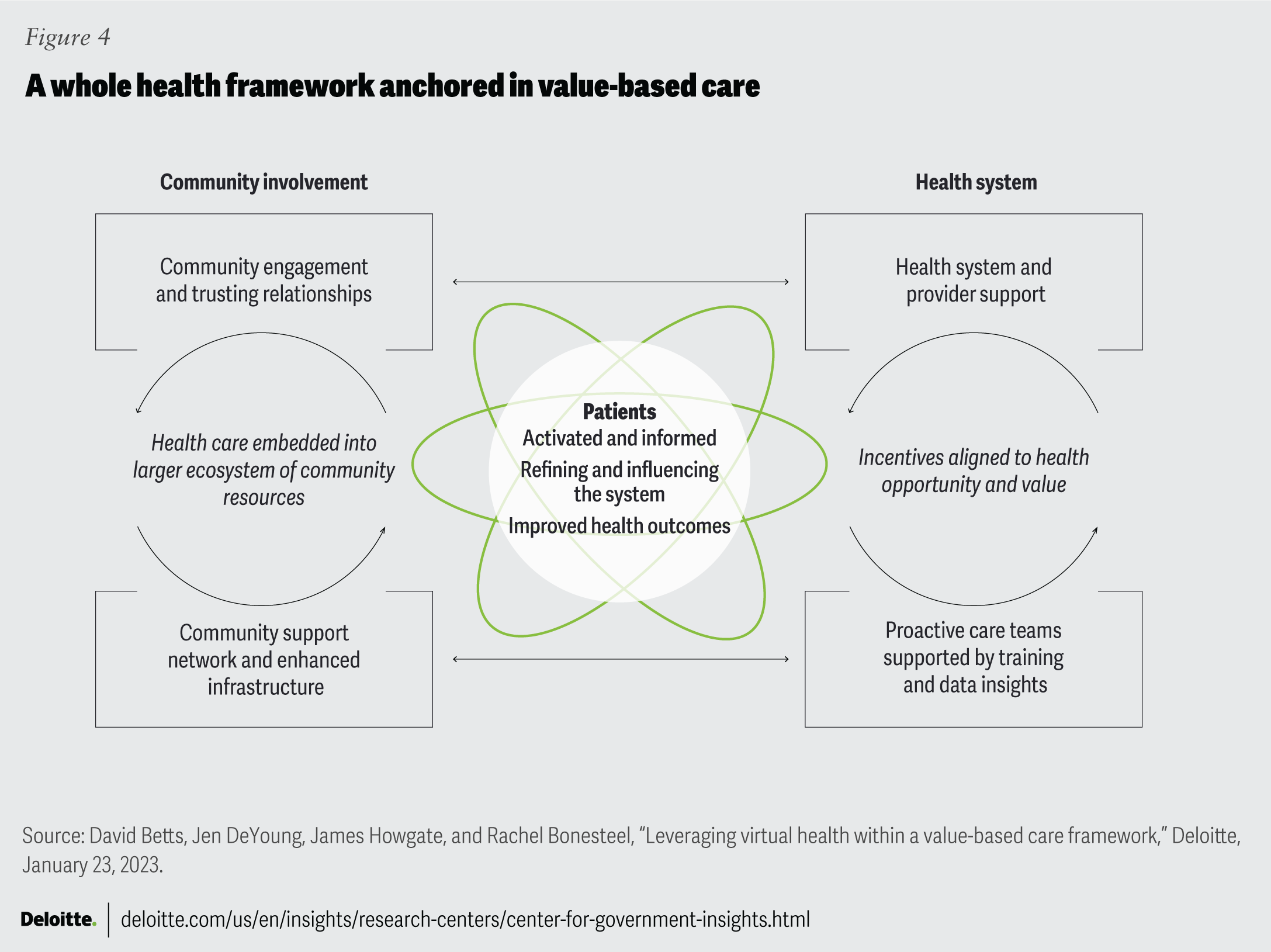
- Prioritize value over volume. Government leaders are helping the industry with its ongoing pursuit to adopt value-over-volume payment models that align incentives with outcomes and value, but there’s more to be done (figure 4).
The state of North Carolina has adopted a payment model that rewards providers who improve population health outcomes at a lower cost of care.35 Between 2019 and 2021, the program saved the state over $155 million.36 It also has generated more than $75 million in revenue for participating health care practices through shared savings allocations and quality bonuses.37 The public-private partnership operates in more than 540 sites; about 85% of those sites are focused on federally designated primary health care provider shortage areas.38 Fair benchmarking will be key as more states work toward value-based care reform.
The state of Maryland, too, is at the forefront of driving innovative health reforms in accountability for health care costs and quality. The state introduced all-payer hospital global budgets, an innovative approach that allocates a fixed annual payment to hospitals, untied to the volume of its services. This paradigm shift incentivized hospitals to actively work toward reducing preventable hospital usage. Maryland succeeded in reducing hospital admissions by 16.2% and reduced differences across several quality measures. From 2019 to 2021, over its first three years, the model reduced total Medicare spending by $689 million.39
{kind=link}
- Create connections across data systems. Establishing interconnected data systems can encourage leaders to make data-driven decisions and focus on not just patient care but the needs of entire populations. Projects aimed at modernizing data and upgrading digital infrastructure can improve both the quality and accessibility of data.
The Chicago Health Atlas uses data-driven information on various health outcomes and indicators in Chicago. Led by the Chicago Department of Public Health in collaboration with partners across multiple sectors in the city, it’s been a resource for over a decade for policymakers, researchers, and the public to better understand differences in health outcomes, access to health care, and other factors impacting public health in the city.40 The resource has also proved useful in times of crisis. When the COVID-19 pandemic hit, the city was able to leverage the Chicago Health Atlas to share data on cases, hospitalizations, deaths, vaccinations, and test positivity without having to build a new platform.
AI and machine learning can also play a role in deriving insights from relatively large, disparate data sets in a short period of time to better understand population health needs, promote health, and prevent disease by identifying geographic risk factors, such as high levels of pollution across a region, as well as protective factors, such as faith institutions or access to fresh, nutritious food. AI can also examine a patient’s medical history, genetics, lifestyle habits, and environmental factors (each being a separate data set) to predict potential health risks. Predictive analytics is capable of revolutionizing government operations and resource allocation, ultimately enhancing public health.41 This can enable early intervention and potentially save lives.42 Public health agencies have already begun utilizing available medical and historical data to make smarter decisions and improve community health.43
- Create whole health by intention and design. Leaders can cocreate the health landscape alongside consumers, patients, families, and those who deliver care. Whole health can be the default approach for government grantmaking and industry investment in research and development, but it can also be used to design community projects and activities to promote health. Intentionality in design, building durable relationships with communities, creating partnerships for continuous measurement, and focusing on both individual- and community-level needs can create whole health by design.44 Meeting people where they are can result in a more complete health transformation that serves the needs of the entire ecosystem.45 This whole health–focused thinking should be prioritized, intentional, and continuous.
Pathways to flourishing: Preparing for change
Today’s health system faces a major challenge: Shifting from the conventional approach of treating diseases and managing symptoms to promoting wellness and healthier and longer lives. The US health care ecosystem can facilitate this transition by forming an interconnected, user-friendly health system. This revamped system could cater to the intricate and interrelated needs of people and communities, leading to improved life span and optimal wellness.
To get there, stakeholders should focus on improving and optimizing the underlying structures, relationships, and dynamics within the health system. By employing a systems-change approach, leaders can identify the interconnections and interdependencies to influence change across the whole system. In this case, that means recognizing that numerous factors shape health outcomes and that health care delivery is not a linear process. Instead, care delivery should be dynamic and adaptive, involving multiple players, feedback loops, and interactions.
Smart regulations could help encourage investments in population health. By balancing innovation and regulations, the government can prioritize a more efficient use of resources. The current emphasis on the volume of services over the value and quality of results has created a disconnect between what health care providers aim for and what patients need. By promoting preventive measures, health promotion, early intervention, and comprehensive care, the ecosystem can improve health care delivery, available treatments, and population results.
The industry has been working toward a value-based care transition for decades, but recent commitments suggest the tide is turning. In 2021, the Centers for Medicare and Medicaid Services established a goal that 100% of original Medicare recipients and the majority of Medicaid recipients would be part of accountable or value-based care arrangements by 2030.46 The changing tides have not gone unnoticed by investors either: One projection estimates value-based care investments will potentially grow from the current $500 billion to $1 trillion.47
As the industry transitions to a value-based care approach, there’s potential to improve care quality, reduce costs, and elevate patient experience and satisfaction. However, continuous data evaluation from health care organizations, providers, and patients is important for consistently delivering high-quality, value-based care. This process entails routinely monitoring and analyzing performance metrics, patient and clinician feedback, and outcomes data to understand the efficiency and efficacy of existing processes, followed by making any necessary adjustments.
Government leaders can help boost value-based care adoption by encouraging access to timely data, reducing administrative burdens, and incentivizing payers to increase base reimbursements for primary care providers. Collaboration is important to building a synchronized and well-coordinated health care system. This can happen at various levels, including between agencies, across different sectors, and through public-private partnerships. Such cooperation can help these entities share information, resources, and expertise to promote innovation, accountability, and trust.
One other piece of the systems change puzzle is human-centered design. This approach centers the design process on the needs, preferences, and experiences of those who use or provide health care services. A health system that is user-friendly and easy to navigate can help meet patients’ needs and empower them to be more involved. Moreover, identifying gaps and pain points that prevent patients from achieving optimal health and well-being fosters an environment of continuous improvement.
Systems change is built upon regulatory change, innovation, collaboration, and human-centered design. The vision is to establish a health system focused on wellness and longevity that can meet the evolving needs of individuals and populations. Over time, this transformation will change how we think about, measure, and invest in health—and ultimately, how we live—for the better.
Continue the conversation
Beth Meagher
Dr. Jay Bhatt
William D. Eggers
By
Dr. Jay Bhatt
Beth Meagher
Alison Muckle Egizi
Rebecca Knutsen
William D. Eggers
The authors would like to thank Nicole Savia Luis and Ipshita Sinha for their research support on this study. The authors would also like to thank Andy Davis, Neal Batra, Grant McLaughlin, Margaret Anderson, Wendy Gerhardt, and Leena Gupta for providing their thoughtful feedback and suggestions at critical junctures.
Cover art by: Jim Slatton and Sofia Sergi; Adobe Stock
Visit the Deloitte Center for Government Insights
Access more insights for the defense, security and justice, government health care, state and local government, transportation and infrastructure, human services, and higher education sectors.
Visit the Deloitte Center for Health Solutions
Access more insights for the hospital, health system and provider, pharmaceutical manufacturer, health plan and payer, medtech, and health tech organization sectors.